Migration from Venezuela:
opportunities for Latin
America and the Caribbean
Regional socio-economic
integration strategy
Migration from Venezuela:
opportunities for Latin
America and the Caribbean
Regional socio-economic
integration strategy
Copyright © International Labour Organization & United Nations Development Programme, 2021
First published 2021
Publications of the International Labour Ofce and the United Nations Development Programme enjoy
copyright under Protocol 2 of the Universal Copyright Convention. Nevertheless, short excerpts from them may
be reproduced without authorization, on condition that the source is indicated. For rights of reproduction or
translation, application should be made to ILO Publishing (Rights and Licensing), International Labour Ofce,
CH-1211 Geneva 22, Switzerland, or by email: [email protected]. The International Labour Ofce welcomes such
applications.
Libraries, institutions and other users registered with a reproduction rights organization may make copies in
accordance with the licences issued to them for this purpose. Visit www.ifrro.org to nd the reproduction rights
organization in your country.
ILO-UNDP Data Catalog
Migration from Venezuela - opportunities for Latin America and the Caribbean: Regional socio-economic
integration strategy. International Labour Organization & United Nations Development Programme, 2021, 68 p.
Labour migration, decent work, employment promotion, informal economy, social protection, Latin America.
ISBN: 978-92-2-034294-7 (print version)
ISBN: 978-92-2-034295-4 (web pdf)
Also available in Spanish:
Migración desde Venezuela: oportunidades para América Latina y el Caribe - Estrategia regional de integración
socioeconómica, ISBN: 978-92-2-033101-9 (print version); ISBN: 978-92-2-033100-2 (web pdf)
The designations employed in ILO and UNDP publications, which are in conformity with United Nations practice,
and the presentation of material therein do not imply the expression of any opinion whatsoever on the part of
the International Labour Ofce and the United Nations Development Programme concerning the legal status of
any country, area or territory or of its authorities, or concerning the delimitation of its frontiers.
The responsibility for opinions expressed in signed articles, studies and other contributions rests solely with
their authors, and publication does not constitute an endorsement by the International Labour Ofce of the
opinions expressed in them.
Reference to names of rms and commercial products and processes does not imply their endorsement by the
International Labour Ofce, and any failure to mention a particular rm, commercial product or process is not a
sign of disapproval.
This document was authored by Adriana Hidalgo and Francesco Carella from ILO, and David Khoudour from
UNDP.
February 2021

The International Labour Organization (ILO) is
mandated to promote decent work for all people
regardless of their nationality. The United Nations
Development Program (UNDP) works with people at
all levels of society to help create nations that can
cope with crises, and lead and sustain the kind of
growth that improves the quality of life of each and
every person. Both organizations joined forces to
develop this Regional strategy for socio-economic
integration.
1 The Regional Platform for Interagency Coordination was formed at the request of the Secretary General of the United Nations on April 12,
2018 to the United Nations High Commissioner for Refugees (UNHCR) and the International Organization for Migration (IOM ) in order to
direct and coordinate the response of the system’s agencies to Venezuelan refugees and migrants, and to complement and strengthen
the countries’ national and regional actions. This response includes meeting the need for protection, assistance and integration of this
population in the host countries of Latin America and the Caribbean. At present, it is made up of international cooperation agencies,
non-governmental organizations, donor agencies and nancial institutions. The Regional Platform is replicated at the national level
through local coordination mechanisms established with the governments.
The Regional strategy was enriched by the
contributions of the agencies that are part of the
Integration Sector of the Coordination Platform for
Refugees and Migrants from Venezuela (R4V
1
) in an
effort to build coherent and complementary proposals
for efforts directed at the migrant population from
Venezuela, including refugees, asylum seekers and
returnees, as well as host communities in the region.
The strategy also contributes to the achievement of
the objectives of the Quito Declaration on Human
Mobility and Venezuelan Citizens in the Region, of
September 2018.
Regional socio-economic integration strategy
5
Context
Since 2015, more than 5.4 million people have had
to leave their country as a result of the economic,
social and political crisis facing Venezuela. Around
85% went to another country in Latin America and
the Caribbean (LAC). This gure, which does not
include hundreds of thousands of returnees, makes
this the most serious migration crisis in the history
of the region.
Often, destination countries view refugees and
migrants as a burden that affects the provision of
public services and the national and local scal
balance. However, international experience shows
that migrants, including refugees, also contribute to
the development of host countries (OECD-ILO, 2018).
Turning migration into a factor for sustainable
development requires that public authorities at
both the local and national levels promote the
socioeconomic integration of the refugee and
migrant population.
Why a Regional Strategy for
socio-economic integration?
While humanitarian aid seeks to meet the basic needs
of the refugee and migrant population, in particular
food, health and housing, a regional economic
integration strategy aims to make its recipients the
promoters of their own subsistence by promoting
their sustainable inclusion in host communities and
their contribution to local economies.
Who is it for?
The Regional Strategy is aimed at the main host
countries for the refugee and migrant population
from Venezuela; in particular, to government
institutions that have some degree of competence in
the socioeconomic integration of this population, and
to employers’ and workers’ organizations, with the
aim of promoting social dialogue around this area.
The countries participating in the Quito Process
identied socioeconomic integration as one of the
priority axes of their work agenda. In addition, the
Regional Response Plan for Refugees and Migrants
from Venezuela (RMRP, 2020), designed within the
framework of the Coordination Platform for Refugees
and Migrants from Venezuela (R4V), includes
socioeconomic and cultural integration among its
four axes for priority action.
Objectives of the Regional
Strategy
The Regional Strategy is oriented towards the
formulation of concrete responses to meet three
objectives:
1. To reduce the levels of socioeconomic vulnerability
of refugees and other migrants from Venezuela.
2. To maximize the contribution of this population to
the economies of the recipient countries.
3. To promote social cohesion through initiatives
that also benet the host communities.
Executive Summary
6
Migration from Venezuela: opportunities for Latin America and the Caribbean
Priority axes of the Regional
Strategy
The Regional Strategy is part of a medium and
long-term framework because it recognizes that the
majority of refugees and migrants from Venezuela
will settle for several years and that the only viable
option for them to contribute to the sustainable
development of their host countries is to promote
socioeconomic integration and coexistence with
their citizens. It is based on international standards
on labour and human rights.
To this end, the Strategy is articulated around seven
priority axes:
i. Regularization and proling of the population
from Venezuela: proposes making more flexible
and expediting the processes of regularization and
proling of the migrant and returned population
and carrying out studies on their demographic
and socioeconomic prole.
ii. Professional training and recognition of
qualications and competencies: seeks to
promote professional training and recognition of
qualications in the region in order to promote
labour inclusion.
iii. Employment promotion: plans to promote
access and efciency of labour intermediation
programs and platforms, boost the employability
of refugees and migrants, and adopt measures
for their transition into the formal economy.
iv. Entrepreneurship and business development:
includes the integration of migrants and refugees
into sustainable entrepreneurship programs
and value chains, as well as promoting self-
employment.
v. Financial inclusion: proposes facilitating access
to nancial services in host countries, promoting
nancial education and adapting banking
services to the needs of the migrant and refugee
population.
vi. Access to social protection, proposes the
preparation of a roadmap to promote a regional
social protection floor and a campaign to
disseminate information on access to social
security.
vii. Social cohesion: foresees the design of
institutional strengthening programs and
awareness campaigns to combat discrimination
and xenophobia.
Strengthening regional
cooperation mechanisms in
matters of the socio-economic
integration of refugees and
migrants into their host
communities
Until now, the Latin American and Caribbean
governments’ response to the Venezuelan migration
crisis has been directed more towards national action
than regional action, although the Quito Process
pursues the latter. For this reason, it is essential that
the countries of the region manage to strengthen
cooperation mechanisms and adopt and implement
truly regional policies, particularly in matters of socio-
economic integration for the refugee and migrant
population that comes from Venezuela, as well as for
host communities.
For the successful implementation of the seven
axes outlined above, it is key that the countries of
the region manage to strengthen their cooperation
mechanisms and adopt regional policies. The
Regional Strategy suggests how to develop and
implement such regional initiatives, focusing on the
areas of:
Regional socio-economic integration strategy
7
i. Human mobility and regularization: better
cooperation in the management of migratory
flows at the regional level and the adoption of
concerted regularization mechanisms to facilitate
intra-regional human mobility and socioeconomic
integration.
ii. Mutual recognition of degrees and
competencies: when a person, whatever their
nationality or immigration status, validates
a technical or academic degree in one of the
countries of the region or certies their labour
competencies, this recognition will be valid in the
other countries of the region.
iii. Labour intermediation: regional cooperation on
labour intermediation implies that both databases
of job vacancies in each country and those of the
job-seeking population, including refugees and
migrants, are shared.
iv. Social protection: the extension of subregional
agreements and promotion of coordination
between national social security laws to guarantee
the access of migrant workers and their families to
national social protection systems and reinforce
the system of portability of rights.
This type of initiative will contribute to a better
response to the protection and inclusion needs of
refugees and migrants from Venezuela at the regional
level in a context aggravated by the COVID-19 crisis.
It will also contribute to the achievement of the
objectives of the Quito Process.
8
Migration from Venezuela: opportunities for Latin America and the Caribbean
Executive Summary
Abbreviations Table
Foreword
Acknowledgments
1. Description
2. Objectives of the Regional Strategy for socio-economic integration
2.1 Why a Regional Strategy for socio-economic integration?
2.2 Applicability and relevance of a Regional Strategy
2.3 Who is the Regional Strategy for and what is expected after its implementation?
2.4 The norms and principles that support and guide the Regional Strategy
a. Technical and declarative instruments
b. Normative instruments of the United Nations System
c. Normative instruments of the Interamerican System for Human Rights
d. Normative instruments of the ILO
3. Socio-labour proling of the population from Venezuela
3.1 Main obstacles to labour insertion
3.2 Distribution and differences by gender
3.3 Main obstacles to labour insertion
3.4 Lack of decent work and job precariousness
3.5 Impact on employment and work due to the measures adopted to stop the spread of
COVID-19
3.6 Social protection in the regional context
4. Priority axes of the regional strategy for socioeconomic integration
4.1 Regularization and proling of the population from Venezuela
4.2 Professional training and recognition of degrees and skills
4.3 Promotion of employment
4.4 Entrepreneurship and business development
4.5 Financial inclusion
4.6 Access to social protection
4.7 Social cohesion
5. Strengthen regional cooperation mechanisms on socio-economic integration
5.1 Expand spaces for collaboration in areas of human mobility and regularization
5.2 Build a regional framework for the mutual recognition of degrees and skills
5.3 Promote labour intermediation at the regional level
5.4 Adopt regional social protection mechanisms
References
Graphics Index
Graphic 1. Percentage of Venezuelans and nationals in the informal sector
Graphic 2. Main areas of regional cooperation in socio-economic integration
Table Index
Table 1. Multilateral mechanisms in the region
Table of Contents
5
9
10
12
14
16
16
17
19
19
20
20
20
20
24
24
25
26
27
29
31
34
34
37
40
44
46
48
51
55
55
57
58
59
61
28
55
18
Regional socio-economic integration strategy
9
Abbreviations Table
LAC Latin America and the Caribbean
ACN Andean Community of Nations
CARICOM Caribbean Community
DTM Displacement Tracking Matrix
OECS Organization of Eastern Caribbean States
OISS Organización Iberoamericana de Seguridad SociaI (Iberoamerican Social Security Organization)
ILO International Labour Organization
IOM International Organization for Migration
PEP Special Residency Permit (Permiso Especial de Permanencia)
PEPFF Permiso Especial de Permanencia para el Fomento de la Formalización (Special Stay Permits
for the Promotion of Formalization)
PTP Permiso Temporal de Permanencia (Temporary Residence Permit)
UNDP United Nations Development Program (UNDP)
RPL Reconocimiento de aprendizajes previos (Recognition of prior learning)
RAMV Registro Administrativo de Migrantes Venezolanos (Administrative Registry of Venezuelan
Migrants)
RMRP Plan Regional de Respuesta para las Personas Refugiadas y Migrantes de Venezuela (Regional
Response Plan for Refugees and Migrants from Venezuela)
SICA Sistema de Integración Centroamericano (Central American Integration System)
10
Migration from Venezuela: opportunities for Latin America and the Caribbean
Foreword
The Latin American and Caribbean region today faces
some of the most acute crises in its history. In order
to face the health crisis and contain the spread of the
COVID-19 pandemic, most governments in the region
have adopted measures for physical distancing and
the restriction of mobility. These have resulted in a
protection crisis for the most vulnerable populations,
particularly those in situations of migration and forced
displacement, as well as a socioeconomic crisis that
has affected people employed in the most vulnerable
sectors of the economy, especially women.
These human development crises were added to
the migration crisis that has plagued the region for
half a decade as a result of the economic, social and
political situation in Venezuela. With more than ve
million Venezuelan refugees and migrants in the
world, around 85% of which are in Latin America and
the Caribbean, the region has to face new challenges
in terms of the mobility of people, access to basic
and protection services, inclusion in labour markets
and social cohesion.
Beyond the humanitarian response aimed at the
population from Venezuela and the host communities,
it is essential that the main recipient countries in the
region consider options to promote socioeconomic
integration and social cohesion. The document
Migration from Venezuela: opportunities for Latin
America and the Caribbean - Regional strategy for
socioeconomic integration seeks to respond to the
increasingly pressing challenge posed by the issue of
migration from Venezuela, particularly in the context
of the COVID-19 pandemic.
Prepared jointly by the International Labour
Organization (ILO) and the United Nations
Development Program (UNDP), within the dual

Regional socio-economic integration strategy
11
framework of the Quito Process and the Coordination
Platform for Refugees and Migrants from Venezuela
(R4V), this document was enriched with inputs from
employers ‘and workers’ organizations, as well as
from the bodies that make up the R4V Integration
Sector. The document Migration from Venezuela:
opportunities for Latin America and the Caribbean -
Regional strategy for socio-economic integration is
structured around seven priority axes: (i) regularization
and proling of the population from Venezuela; (ii)
professional training and recognition of degrees and
skills; (iii) job promotion; (iv) entrepreneurship and
business development; (v) nancial inclusion; (vi)
access to social protection; and (vii) social cohesion.
Since these efforts need to be part of a logic of
cooperation, the Regional Strategy proposes the
adoption of concerted mechanisms to facilitate
regional mobility and regularization of the population
in an irregular situation to promote the mutual
recognition of degrees and skills, develop initiatives
that improve labour intermediation at the regional
level, guarantee the access of refugees and migrants
to social protection systems and reinforce the
portability of acquired rights.
The unprecedented challenges faced by our region
require a coordinated response to build more
peaceful, just and inclusive societies, with decent
work, that take into account not only the needs and
vulnerabilities of refugees and migrants, but also
their contributions to the sustainable development of
the region. With this objective, our two organizations
are ready to support regional bodies as well as
national and local authorities in Latin America and
the Caribbean in the implementation of the measures
developed within the framework of this Regional
Strategy.
Vinícius Carvalho Pinheiro
Assistant Director-General of the ILO
Regional Director for
Latin America and the Caribbean International
Labour Organization
Luis Felipe Lopez-Calva
Sub-Secretary-General of the UN
Regional Director for
Latin America and the Caribbean United Nations
Development Programme
12
Migration from Venezuela: opportunities for Latin America and the Caribbean
This Regional Strategy is the result of a collaboration
between the International Labour Organization (ILO),
the United Nations Development Program (UNDP),
the different agencies that make up the Coordination
Platform for Migrants and Refugees from Venezuela
(R4V) and the member countries of the Quito Process.
The document was drafted by Adriana Hidalgo and
Francesco Carella from the ILO and David Khoudour
from UNDP, under the direction of Vinícius Carvalho
Pinheiro, ILO Regional Director for Latin America and
the Caribbean, José Cruz-Osorio, Director the UNDP
Regional Centre for Latin America and the Caribbean,
and Jairo Acuña-Alfaro, Leader of the Governance
Team of the same Regional Centre.
The document also beneted from the valuable
contributions of the members of the R4V Platform,
led by the UNHCR and IOM, and especially those
partners that make up the Integration Sector.
Likewise, the support of the member countries
of the Quito Process was of great importance, in
particular the pro témpore Presidencies of Colombia,
Peru and Chile, as well as the representatives of the
organizations of workers and employers of the region,
who contributed signicantly to the development of
this document.
Finally, it is important to highlight the collaboration
and contributions of the participants of the different
spaces where this Regional Strategy was socialised,
among which the Technical Seminar with the
Integration Sector of the R4V Platform held on May
19, 2020, stands out, along with the Workshop on
Socio-economic Integration and follow-up to the
Recommendations of the Meeting of Ministers of
Labour of the Quito Process, held on August 20, 2020.
Acknowledgments

Regional socio-economic integration strategy
13
1
Description
The current Venezuelan migration crisis is the worst ever seen in the history
of Latin America and the Caribbean (LAC). Since 2015, more than 5.4 million
Venezuelans have had to leave their country as a result of the economic,
social and political crisis facing Venezuela. This gure, which does not include
hundreds of thousands of returnees, makes it the second largest migration
crisis in the modern world, after the Syrian crisis.

14
Migration from Venezuela: opportunities for Latin America and the Caribbean
About 85% of Venezuelan refugees and migrants
moved to another country in the LAC region.
Colombia is the country that is receiving the highest
numbers of people. As of August 5, 2020, this
country welcomed 1.8 million Venezuelans (35.8%
of the entire Venezuelan population in a situation of
mobility), as well as an estimated number of at least
500,000 Colombian returnees from Venezuela. They
are followed by Peru (830 thousand people), Chile
(455 thousand) and Ecuador (363 thousand). Brazil
(265 thousand) is the sixth largest recipient country
for the Venezuelan population, just after the United
States (351 thousand) and before Argentina (179
thousand) (R4V, 2020).
For their part, Aruba (16%), Curaçao (10.1%),
Colombia (3.6%), Panama (2.9%) and Guyana (2.8%)
are the main recipient countries as a percentage of
the host population. This implies that these countries
are the ones with the greatest pressure in terms
of humanitarian assistance, provision of public
services, access to jobs and citizen coexistence. In
other countries in the region, such as Brazil, Mexico
and Paraguay, the Venezuelan population represents
only 0.1% of the total. Their absorption capacities are
higher, while the costs associated with the integration
of the Venezuelan population are lower than those
of host countries with a higher concentration of
Venezuelan population.
In the region, many destination countries tend to view
refugees and migrants from Venezuela as a burden
that affects the provision of public services and the
national and local scal balance, not to mention
the challenges in terms of cohesion and peaceful
coexistence. However, international experience
shows that immigrants, including refugees, also
contribute to the development of their host countries
(OECD-ILO, 2018). On the one hand, they represent
a source of human capital that makes it possible to
respond to the labour shortage in some sectors of
the economy. They also invest and consume, which
2 “A economía de Roraima e o fluxo venezuelano”. Fundação Getulio Vargas - Diretoria de Análise de Políticas Públicas (FGV-DAPP),
ACNUR, Observatório das Migrações Internacionais (OBMigra), Universidade Federal de Roraima (UFRR) y ACNUR.
contributes to feeding aggregate demand and thus
GDP growth. On the other hand, by paying taxes,
directly and indirectly, the refugee and migrant
population contributes to improving the scal
balance of their host countries.
An example of the positive effects on the local
economy was evidenced in a study on the impact
on society and the economy of the arrival of
Venezuelans to Roraima, Brazil. This municipality
registered growth and economic diversication
during the period of highest influx
2
. Likewise, the
tax receipts generated in 2018 by all Venezuelans is
comparable to the additional expenses required for
their acceptance, with both gures in the range of R
$ 100 million.
Turning migration into a factor for sustainable
development requires that public authorities,
both at the local and national levels, promote the
socioeconomic integration of the refugee and
migrant population. This is precisely the purpose of
this Regional Strategy. The health, economic and
social crisis generated by the COVID-19 pandemic
makes it an even more necessary tool.

Regional socio-economic integration strategy
15
2
Objectives of the
Regional Strategy
for socio-economic
integration
The Regional Response Plan for Refugees and Migrants from Venezuela (RMRP,
2020) includes socio-economic and cultural integration among the priority
lines of action of the Coordination Platform for Refugees and Migrants from
Venezuela (R4V). It also highlights the fact that “effective socio-economic
and cultural integration is favourable not only for refugees and migrants from
Venezuela, but also for host communities.”
16
Migration from Venezuela: opportunities for Latin America and the Caribbean
Likewise, within the framework of the Meeting of
Ministries of Labour in support of the Quito Process,
in Bogotá, Colombia (November 13, 2019), the
representatives of different Ministries of Labour
of Latin America and international cooperation
organizations insisted on the need to “promote
socio-economic integration with an emphasis on
access to the labour market for refugees, migrants
and returnees from Venezuela in Latin America and
the Caribbean through collaborative work with the
different international cooperation organizations and
agencies within the decent work framework. ” They
also recommended “cooperating with the design of
an income generation strategy for refugees, migrants
and returnees from Venezuela, linked to migration
policies, which contributes to the formalization of
work and progressive access to a social protection
floor.”
The Regional Strategy for Socio-economic Integration
constitutes a concrete response to this dual concern of
the Coordination Platform for Refugees and Migrants
from Venezuela and of the Ministries of Labour of the
member countries of the Quito Process. Not only is
it part of a humanitarian logic of reducing the levels
of socioeconomic vulnerability of refugees and other
migrants who come from Venezuela, but it also seeks
to maximize the contribution of this population to the
economies of the recipient countries and promote
social cohesion through initiatives that also benet
the host communities.
2.1 Why a Regional Strategy
for socio-economic
integration?
While humanitarian aid seeks to satisfy the basic
needs of the refugee and migrant population, in
particular food, health and housing, an economic
integration strategy aims to support the recipients
in becoming actors of their own subsistence. In this
sense, it is a recognition that “there is a growing
need to strengthen the link between humanitarian
assistance and development in the global response
and to place employment in a strategic place
between both components” (ILO, p. 12, 2016). It also
responds to the need to develop or strengthen labour
market institutions and programs that support local
integration, resettlement, voluntary repatriation and
reintegration, as reafrmed in the ILO’s Guiding
Principles: Access of refugees and other forcibly
displaced persons to the labour market.
Refugees and migrants from Venezuela face a series
of obstacles that hinder their integration into the
region’s labour markets or prevent them from creating
their own businesses. The lack of a regular status
represents one of the biggest obstacles to getting
a formal job or starting a business. However, those
in a regular situation also have difculties accessing
decent jobs and obtaining recognition of their
academic degrees and professional skills. Accessing
opportunities to develop skills and competencies
that allow them to be more competitive in the
labour market represents an additional obstacle.
The population from Venezuela, including returnees,
also faces discrimination problems and a high risk
of labour exploitation. This situation is even more
acute in the case of vulnerable populations, such
as women, ethnic minorities and disabled people,
among others.

Regional socio-economic integration strategy
17
In this sense, the Regional Strategy describes the
main ways to promote socioeconomic integration
with special consideration for women, who face more
precarious labour insertion conditions and greater
risks of violence and sexual and labour harassment
for gender reasons, among other realities.
The health, socioeconomic and care crisis generated
by COVID-19, as well as the physical distancing
measures that have been taken throughout the
region, aggravated the migratory crisis and increased
the risks of rejection towards people from Venezuela.
Within the host communities, many people already
experienced situations of poverty, hunger and
exclusion. For this reason, promoting socioeconomic
integration implies thinking about sustainable
development strategies that consider the community
as a whole, and that can and should benet everyone.
A strategy that is exclusively oriented towards the
refugee and migrant population could contribute
to increasing the frustration of the local population
and represent a factor for rejection, especially in the
current context of COVID-19.
From this perspective, the Regional Strategy for
socioeconomic integration is structured around
seven axes:
1. Regularization and proling of the population
from Venezuela
2. Professional training and recognition of
qualications and skills
3. Job promotion
4. Entrepreneurship and business development
5. Financial inclusion
6. Access to social protection
7. Social cohesion
3 International Labour Organization. ILO Declaration on Fundamental Principles and Rights at Work. See: https://www.ilo.org/declaration/
lang--es/index.htm
Each country will be able to position itself in relation
to this Regional Strategy based on its specic needs
and progress on the seven aforementioned axes,
but always within a framework of respect for human
rights and international labour standards, in particular
the fundamental principles and rights at work
3
. The
participation of the social partners (employers’ and
workers’ organizations) in a tripartite social dialogue
with the Government is very important to dene the
specic adaptations to guide this Strategy in each
national context.
2.2 Applicability and relevance
of a Regional Strategy
When targeting diverse countries, a Regional Strategy
poses the challenge of applicability, adaptability and
relevance. Among the challenges, these factors
should be recognized above all:
} The global socio-economic context derived from
the effects of the pandemic caused by COVID-19
and the quarantine and social distancing
measures adopted by each country.
} The different institutional capacities of each
country.
} That the countries are at different stages of
development to respond to the needs and
demands of the target population of this Regional
Strategy.
Faced with these divergences, an added value of
the regional proposal is to seek that the countries
give each other feedback through the exchange of
good practices and lessons learned. Membership in
regional mechanisms facilitates a more articulated
response (see Box 1).

18
Migration from Venezuela: opportunities for Latin America and the Caribbean
Regional collaboration within the Quito Process,
as well as the support of the different actors of the
Coordination Platform for Refugees and Migrants
from Venezuela (R4V), also constitutes an added
value for the successful implementation of the
Regional Strategy for socio-economic integration.
Southern Common Market (MERCOSUR)
●Multilateral Agreement on Social Security (1997).
Agreement on Residence for Nationals of MERCOSUR Member States and Agreement on Residence for Nationals
of MERCOSUR Member States, Bolivia and Chile.
Plan to Facilitate the Free Movement of Mercosur Workers (2013
Andean Community of Nations (ACN): Bolivia, Colombia, Ecuador and Peru
Andean Instrument for Labour Migration (2003) - Participants: Colombia, Ecuador and Peru.
Andean Instrument for Labour Migration (Decision 545).
Resolution 957: Regulation of the Andean Instrument for Safety and Health at Work.
Pacic Alliance
Its creation, via the Declaration of Lima (2011), established the purpose of progressively advancing towards “the
free movement of goods, services, capital and people,” to prioritize “the movement of business people and facilitate
migratory transit including migratory cooperation and consular police.”
Caribbean Community (CARICOM)
●Members: Antigua and Barbuda, The Bahamas, Barbados, Belize, Dominica, Grenada, Guyana, Haiti, Jamaica,
Monserrat, Saint Lucia, Saint Kitts and Nevis, Saint Vincent and the Grenadines, Suriname, and Trinidad and
Tobago.
Agreement on Social Security (2006).
Central American Integration System (SICA)
The Central American Social Integration Treaty (Treaty of San Salvador, 1995) aims to achieve Central American
social integration through the coordination, harmonization and convergence of national social policies, for which
purpose the Social Integration Subsystem was created and the Central American Social Integration Secretariat
(SISCA) was established.
Ibero-American Social Security Organization (OISS)
●Ibero-American Multilateral Agreement on Social Security.
Table 1. Multilateral mechanisms in the region

Regional socio-economic integration strategy
19
2.3 Who is the Regional
Strategy for and what
is expected after its
implementation?
The Regional Strategy is directed at the governments
of the main host countries for refugee and migrant
populations that come from Venezuela, especially
government institutions that have some degree of
competence in their socio-economic integration.
It draws on the Colombian experience, where the
Venezuelan Border Management of the Presidency of
the Republic, with the support of UNDP, designed an
income generation strategy for the migrant population
from Venezuela and the host communities (UNDP /
Presidency of the Republic of Colombia, 2019).
Following the implementation of the Strategy, the
population from Venezuela, as well as members of
the host communities, especially those affected by
the health, socioeconomic and care crisis induced by
COVID-19 are expected to:
} Benet from a regular immigration status that
allows them, among other things, to have access
to public or reasonably priced health services,
education, care and nancial services, as well as
to develop new skills and manage the recognition
of their degrees and skills, insert themselves into
the labour markets of the host countries and
create their own businesses.
} Have access to salaried jobs or under the
modality of self-employment in the formal sector
of the economy, with full exercise of their labour
rights and in observance of health and safety
regulations at work, as well as those referring to
the minimum age of admission to employment.
4 This guarantee of access to a minimum level of social protection must be articulated within the framework of a broader strategy of
extension of coverage through an integrated policy approach and access to higher levels of social protection in line with Convention No.
102 of the ILO on the minimum standard of social security.
} Benet from a social protection floor against a
state of need or social vulnerability that requires
the intervention of the different non-contributory
programs, to guarantee access to a basic level
of social protection. This floor will allow, as a
minimum, that they have access throughout
their life cycle to essential health care and basic
income security that, in turn, will enable them
to have effective access to goods and services
dened as necessary at the national level
4
.
2.4 The norms and principles
that support and guide the
Regional Strategy
The recommendations included in this document are
part of the global agenda on migration, particularly
labour, forced displacement and sustainable
development. They are based on the guiding principles
dened in the Global Compact for Safe, Orderly and
Regular Migration (UN, 2018a), the Global Compact
on Refugees (UN, 2018b) and the 2030 Agenda for
Sustainable Development (UN, 2015). The Regional
Strategy follows the guiding principles of human
rights and a gender perspective and adopts a pan-
governmental and pan-social approach.
Likewise, there is a migration governance framework
at the international level that is made up of binding
and non-binding normative instruments, guiding
technical instruments for the denition of national
policies, and others that meet universal aspirations.
These are included in the basis of this Regional
Strategy, but it is also hoped that the countries that
have not ratied them - where appropriate - move
towards this process and that, in all cases, their
content is disclosed and implemented.
20
Migration from Venezuela: opportunities for Latin America and the Caribbean
Those that are most closely related to the dimensions
addressed by this strategy are listed below,
recognizing that the list can be much longer:
a. Technical and declarative instruments
ILO multilateral framework for labour migration.
Non-binding principles and guidelines for a
rights-based approach to labour migration
(2007).
High-Level Dialogue on International Migration
and Development (2013). General Assembly of
the United Nations.
2030 Agenda for Sustainable Development
(2015). General Assembly of the United
Nations.
The “Guiding principles on the access of
refugees and other forcibly displaced persons
to the labour market” (2016).
General principles and guidelines for fair
recruitment and Denition of recruitment fees
and related expenses (2016 and 2018).
Global Compact for Safe, Orderly and Regular
Migration (2018).
Global Compact on Refugees (2018).
Declaration of Panama. 19th American
Regional Meeting of the ILO (2018).
ILO Centenary Declaration on the Future of
Work (2019). International Labour Conference,
One Hundred and Eighth Session to mark the
Centenary of the ILO.
Resolution on the ILO Centennial Declaration
on the Future of Work (adopted on June 21,
2019).
b. Normative instruments of the United
Nations System
Convention on the Elimination of All Forms
of Discrimination against Women (1979).
General Assembly of the United Nations.
International Convention on the Protection
of the Rights of All Migrant Workers and
Members of Their Families, adopted by
the United Nations General Assembly in its
resolution 45/158, of December 18, 1990.
Convention on the Status of Refugees, adopted
on July 28, 1951 by the Plenipotentiary
Conference on the Status of Refugees and
Stateless Persons, convened by the General
Assembly of the United Nations.
Protocol on the Status of Refugees, signed
on January 31, 1967 at the United Nations
General Assembly.
c. Normative instruments of the Interamerican
System for Human Rights
Convention on Political Asylum (1933).
Inter-American Convention on the Prevention,
Punishment and Eradication of Violence
against Women or “Convention of Belem do
Pará” (1994).
Convention on Diplomatic Asylum (1954).
Convention on Territorial Asylum (1954).
Additional Protocol to the American Convention
on Human Rights in the area of Economic,
Social and Cultural Rights or “Protocol of San
Salvador” (1988).
Inter-American Convention Against all Forms
of Discrimination and Intolerance (2013).
d. Normative instruments of the ILO
The fundamental ILO conventions are listed, so
named because they are a prerequisite for the
development of subsequent governance conventions
and considered a priority due to their relevance to
the operation of the international labour standards
system. Other conventions and recommendations
that address the components of this strategy
(employment, social protection, rights of migrant
workers and development of human resources,
among others) are also considered.
Regional socio-economic integration strategy
21
d.1 Core conventions
Forced Labour Convention, 1930 (No. 29)
and its Protocol of 2014 to the Forced Labour
Convention, 1930.
Freedom of Association and Protection of the
Right to Organize Convention, 1948 (No. 87).
Right to Organize and Collective Bargaining
Convention, 1949 (No. 98).
Equal Remuneration Convention, 1951 (No.
100).
Abolition of Forced Labour Convention, 1957
(No. 105).
Discrimination (Employment and Occupation)
Convention, 1958 (No. 111).
Minimum Age Convention, 1973 (No. 138).
Worst Forms of Child Labour Convention,
1999 (No. 182).
d.2 (Priority) governance conventions of the ILO
Labour Inspection Convention, 1947 (No.
81); Protocol of 1995 relating to the Labour
Inspection Convention, 1947.
Employment Policy Convention, 1964 (No.
122).
Labour Inspection (Agriculture) Convention,
1969 (No. 129).
Tripartite Consultation (International Labour
Standards) Convention, 1976 (No. 144).
d.3 Other applicable ILO conventions and
recommendations
Conventions
Preservation of Migrants’ Pension Rights
Convention, 1935 (No. 48).
Employment Service Convention, 1948 (No.
88).
Migrant Workers Convention (Revised), 1949
(No. 97).
Social Security (Minimum Standards)
Convention, 1952 (No. 102).
Plantations Convention, 1958 (No. 110) and
its Protocol of 1982 relating to the Plantations
Convention, 1958.
Equality of Treatment (Social Security)
Convention, 1962 (No. 118).
Employment Injury Benets Convention, 1944
(No. 121).
Invalidity, Old-Age and Survivors’ Benets
Convention, 1967 (No. 128).
Medical Care and Sickness Benets
Convention, 1969 (No. 130).
Human Resources Development Convention,
1975 (No. 142).
Migrant Workers (Supplementary Provisions)
Convention, 1975 (No. 143).
Workers with Family Responsibilities
Convention, 1981 (No. 156)
Preservation of Social Security Rights
Convention, 1982 (No. 157).
Employment Promotion and Protection
against Unemployment Convention, 1988 (No.
168).
Private Employment Agencies Convention,
1997 (No. 181).
Maternity Protection Convention, 2000 (No.
183).
Domestic Workers Convention, 2011 (No. 189).
Violence and Harassment Convention, 2019
(No. 190).
Recommendations
Livelihoods Security Recommendation, 1944
(No. 67).
Medical Care Recommendation, 1944 (No. 69).
Migrant Workers Recommendation (Revised),
1949 (No. 86).
Migrant Workers Recommendation, 1975 (No.
151).
Social Protection Floors Recommendation,
2012 (No. 202).
Transition from the Informal to the Formal
Economy Recommendation, 2015 (No. 204).
Employment and Decent Work for Peace and
Resilience Recommendation, 2017 (No. 205).
Violence and Harassment Recommendation,
2019 (No. 206).
22
Migration from Venezuela: opportunities for Latin America and the Caribbean
The Regional Strategy is established within this
regulatory framework and is based on the following
principles:
All of the actions implemented include both
the refugee and migrant population, including
returnees, as well as the host communities,
unless for some reason their application is
specied only for one or the other.
It is recognized that refugees enjoy a different
protection status under international law.
Respect for human rights in general and
labour rights in particular are guaranteed for
all working people in a situation of mobility.
Tripartite social dialogue is promoted in the
debate on and denition of the governance
frameworks for labour migration.
The actions for implementing the Strategy
include the promotion of decent work, both in
the urban and rural sectors.
The exercise of freedom of association
and collective bargaining is recognized and
guaranteed.
It is based on and promotes equal opportunities
and treatment in employment, as well as
respect for diversity.
The right of minors to live free from child
labour and hazardous work.
The right of people to live free from forced
labour.
The promotion of a national social protection
floor, which guarantees income security
throughout the entire life cycle and effective
access to essential health services,
accompanies measures to promote socio-
economic integration because this constitutes
one of the elements required for decent work.
It is formulated from a gender and
intersectional perspective that considers the
relevance of the service offer according to
the life cycle and the business cycle, which
guides actions and strategies, and recognizes
the different experiences faced by women in
terms of barriers to socioeconomic inclusion
and, in particular, those related to care needs
and responsibilities for families, which usually
falls on migrant women.

Regional socio-economic integration strategy
23
3
Socio-labour proling
of the population from
Venezuela
Socio-economic integration is essential for the population from Venezuela,
who need stable sources of income to sustain themselves in their new location
and send remittances to their families. However, despite the fact that the
majority of Venezuelans and returnees are of a productive age and have a high
educational prole, they face many challenges when entering the labour market
under decent working conditions.

24
Migration from Venezuela: opportunities for Latin America and the Caribbean
3.1 Age and educational prole
According to various studies, the majority of refugees
and migrants from Venezuela are young, between 18
and 35 years old, with the group between 26 and 35
years old being the largest, followed by the group
of people between 18 and 25 years old. Salgado et
al. (2017) point out that in Chile, the population of
Venezuelans is young and in full productive capacity
because they belong to the age range of between 20
and 35 years old and, to a lesser extent, in the range
of 36 to 50 years, with an average of 29.2 years.
Similarly, Simoes, Cavalcanti, Moreira and Camargo
(2018) point out that in Brazil, Venezuelan immigrants
are mostly young (72% are between 20 and 39 years
old). Ramírez et al. (2019), and further establish that
in Ecuador, 55% of the Venezuelan population is in
the age range between 18 and 35 years.
An analysis of the most recent reports of the
IOM Displacement
5
Tracking Matrix (DTM) for
the countries of Latin America and the Caribbean
corroborates these results. In Panama, 83% of the
Venezuelan people surveyed are in the age range
of 18 to 45 years, with a higher concentration in the
ages of 26 to 35 years (DTM September 2019); in
Trinidad and Tobago, the majority are between 25
and 29 years old, followed by the group of people
between 30 and 34 years old (DTM September 2018).
The analysis of these same reports makes it possible
to verify that Venezuelans with higher educational
levels migrate to the Southern Cone of America,
Panama, Mexico, Costa Rica and the Dominican
Republic, while those with technical and secondary
educational proles (mostly complete) tend to migrate
to the Andean countries, Brazil and the Caribbean
countries of Aruba, Curaçao, Trinidad and Tobago,
5 The Displacement Tracking Matrix (DTM) is IOM’s global tool for capturing, processing and generating information on the movements
of people in different countries. Specically, they are surveys of people over 18 years old that are carried out at border points and
destination cities. They provide information on the prole of people in human mobility, transit routes, living and working conditions, as
well as the particular vulnerabilities and specic needs they face.
6 According to a report on the RV4 Platform, there were three shipwrecks that caused more than 80 deaths of Venezuelans who were
taking the sea route to Caribbean countries (RV4 April-May 2019).
and Guyana. This is presumed to happen because
those with a higher occupational qualication
migrate to countries that are perceived to have
better and greater job opportunities (Bravo and Úzua,
2018; Koechlin, Solórzano, Larco and Fernández-
Maldonado, 2019). It also follows that, due to their
socioeconomic prole, the rst group corresponds
to people with the ability to travel to more distant
destinations since, according to the DTM analysed,
those who migrate to the Southern Cone, Panama,
Mexico, Costa Rica and the Dominican Republic
make all or part of the trip by plane while those who
travel to neighbouring or closer countries make part
of their trip by bus, boat
6
and / or on foot.
However, some differences between the rst and
second migratory waves can be identied. The
rst migrations corresponded mainly to people
with postgraduate, university and higher technical
studies, including professionals in careers such
as Engineering, Social Sciences, Administrative
Sciences, Education, Medicine and Law, among
others (Mercer, 2019; Tincopa et al., 2019; Salgado
et al., 2017). The most recent waves include younger
people with less education and little work experience.
In other words, recent migrations are of people who
leave the country in conditions of greater vulnerability
and with less work experience (Blouin, 2019).
Regional socio-economic integration strategy
25
3.2 Distribution and differences
by gender por género
Women represent about half of the people who
come from Venezuela and, on average, have higher
educational levels than their male counterparts;
they also have work experience. It is estimated that
more than 70% worked before migrating and of
these, approximately 57% had a formal job, a similar
proportion to their male counterparts, while 16% were
unemployed (9% of men were) ( IOM, 2018).
Despite this, they face signicantly worse job
placement conditions than men. Unemployment
is generally double what they experienced before
they migrated and at least double that of their male
counterparts. These results are influenced by the
combination of the sexual division of labour within
households and in labour markets, and the violence
experienced in transit and destination (Carcedo,
Chaves Groh and Larraitz Lexartza, 2020).
Within households, the migratory experience tends
to reinforce, reproduce and increase the differences
in the distribution of care work and other unpaid
tasks. Women who come from Venezuela take care
of the family more intensively than before migrating
and do so more than men. This difference tends
to grow in the places of destination, where the
difculties of educating the little ones, the lack of
care services and support networks, and the scarcity
of resources that prevent hiring third parties for
household tasks lead women to disproportionately
assume reproductive responsibilities within families.
To meet this demand, they also do not have the
help of the extended family and, in particular, of
older women; less than 10% of women are over
50 years old. For women heads of households,
the pressure is even greater (Carcedo et al., 2020).
In LAC countries, the sexual division of labour outside
the home produces labour markets with strong
segmentation and horizontal segregation by sex, which
implies a high concentration of women in professions
and trades that require fewer qualications (ECLAC,
2019). These markets favour the disqualication of
women who come from Venezuela and reinforce
precarious work in jobs that are usually located within
the informal economy and, therefore, in working
conditions with a lack of decent work. Among
these are occupations related to cleaning, caring
for other people, and street vending. In fact, women
reach a labour market that is already segregated
by sex, but they only manage to insert themselves
into feminized and low-productivity occupations.
They are not successful in entering occupations
where women are the majority, but require high or
medium-high qualications, such as health and
education. For many, this segmentation of the labour
market implies giving up their professions and work
experiences and reinforces their disproportionate
participation in the care economy in two ways:
inside and outside their homes, paid and unpaid.
The violence and harassment experienced by women
and girls of all ages who come from Venezuela also
impact their access to livelihoods and contribute to
their exclusion from labour markets, which implies
loss of employment, lack of incentive to search and
consequent real access only to jobs with high levels
of risk. Street sales, domestic work and sex work are
some of the sectors in which migrant women nd
employment opportunities and, at the same time,
risk situations, as well as exposure to violence and
exploitation.
The reinforcement of the domesticity mandate
reaches not only the loss of their professions,
businesses or disconnection from the collective
spaces in which they were reafrmed, they also lose
the possibility of acting and interacting on their own
behalf in different settings and with different people.
This drastic change, the lack of job opportunities and
precarious living conditions, as well as an increase in
reproductive workloads and the risks of sexual, sexist
and xenophobic violence reinforce this enormous
decline in their quality of life.

26
Migration from Venezuela: opportunities for Latin America and the Caribbean
3.3 Main obstacles to labour
insertion
In general, refugees and migrants from Venezuela,
especially women, nd more opportunities to
be employed in the informal economy, with the
limitations it implies in terms of access to labour
rights. The reason is structural: between half and
three-quarters of the jobs in Latin America and
the Caribbean are in the informal economy, either
because they are jobs without a formal contract and
in precarious conditions or because they include low-
productivity enterprises and, therefore, do not offer
the possibility of affording coverage against various
risks of the present and future (ILO, 2019).
In Peru, the study by Koechlin et al. (2019) points
out that the insertion of Venezuelan people into
employment “has been at the cost of reinforcing
the predominant tendencies of the Peruvian
occupational structure, that is, the generation of
employment in the informal sector of the economy”
(2019, pp. 50 -51). In its study on immigration of
South Americans in Argentina, the ILO (2011, p. 123)
indicates that these people are inserted in “(…) a
labour market characterized by the high presence of
precarious jobs for the population as a whole, where
the migrant population takes the worst part (…). ” The
insertion of the migrant population into the labour
market is determined, therefore, by its structure and,
in this case, by informality, clearly to the detriment
of compliance with labour rights. In Trinidad and
Tobago, more than 90% of Venezuelans surveyed for
7 The delays in obtaining an appointment to start the application for the residency procedure in Argentina are up to 12 months. On the
other hand, in May 2018, the Argentine Executive increased the prices of all administrative immigration fees, including the fee to request
an urgent appointment that increased ve times from 2,000 to 10,000 Argentine pesos (from 47 to 234 euros) (Pacecca, 2018, in Acosta
et al., 2019).
8 In Panama, among the different challenges to regularizing or applying for refugee status, the DTM report indicates: (1) the expiration
/ theft / loss of passport (Venezuelan people are not accessing new documents either in the consulates or in Venezuela) although,
on occasions, they receive consular certicates of passport extension for the immigration and labour regularization procedures; (2)
the cost of immigration regularization and legal representation. Additional costs include the processing and sending of documents to
Venezuela, payment to the responsible person in Panama and travel / stay in the capital for those who live in the interior of the country
(DTM September 2019, p. 15).
9 In Ecuador, where neither documents nor extenuating circumstances are required, the main limiting factor to obtaining documentation
is the cost. The visa application costs 50 USD; the UNASUR Visa costs 250 USD, and the temporary visa costs 400 USD (Ministry of
Foreign Relations, 2019, in Célleri, 2010, p. 13).
the DTM report indicated that they were working in
the informal sector (DTM September 2018).
In relation to immigration regulation, the processes
involved are long and expensive, and in some cases
access to it is impossible. Not having a regular
immigration status constitutes a limitation for access
to decent work, as already outlined by various studies
(Tincopa, 2019
7
; Acosta et al., 2019
8
; DTM Panama
2019; Célleri, 2019
9
). In the Dominican Republic, the
DTM report indicates that, “although the Venezuelan
population nds activities that generate income,
these are low. There is limited access to labour rights
due to their irregular migration status ”(DTM October-
November 2018). In a study carried out with women
in Peru, the results of which can be extrapolated
to men, the following were identied as obstacles
to labour insertion: (1) the difculty of requesting
appointments at the National Directorate of Migration,
which leads women to resort to “processors” (people
who can access the website at dawn to process an
appointment); (2) the existence of few State ofces
for managing immigration documents, such that
women have to stand in long lines to obtain them;
and (3) high costs, such as for the Interpol File and
the immigration card (Tincopa, 2019).
Having a document proving one’s refugee status or
a work permit is not a guarantee of access to the
job market. There are some barriers that are related
to the lack of information on the part of the private
sector about this migratory category, since they
do not know whether these documents are valid
and are not sure of the existence of restrictions to
Regional socio-economic integration strategy
27
hiring migrants, such as work permits for certain
occupations.
Access to vocational training in the LAC region is
usually conditioned on the possession of immigration
documentation and, in general, a residence card and
a basic level of education are required according
to the policies of vocational training institutes.
Sometimes, as previously mentioned, migrants and
refugees do not carry their diplomas and, therefore, it
is impossible to demonstrate the minimum required
degree, which makes it impossible to access these
alternatives to strengthen employability. In countries
like Costa Rica, people between the ages of 15 and
17 can access the courses available at the Instituto
Nacional de Aprendizaje (INA), regardless of their
immigration status. Access facilities for this type
of training promote job placement under more
favourable conditions, because they allow access to
degrees that prove mastery of certain skills.
The validation of university degrees requires going
through tedious processes (obtaining apostilles
or nding documents that are not available in
Venezuela), that are long and expensive. In many
cases, the document that they do not carry or that
they cannot obtain is the diploma itself: “despite the
fact that 40% of the Venezuelan people surveyed
have higher education, only half have been able to
bring their diploma to Peru (50 %). Of this group, only
half have validated their diploma (50%) ”(Blouin, 2019,
p. 58). A related problem is the inability to obtain
documents in Venezuela when requested.
The costs also represent an obstacle because “the
Venezuelan migrant must debate whether to assume
the costs of validating professional degrees or
whether to save that money for survival purposes or
for sending remittances” (Blouin, 2019, p.59). This
situation generates a low correspondence between
their studies (university or technical-superior) and
the type of work they perform.
Koechlin et al. (2019), in their study on labour
insertion in Peru, asked what is the relationship
between the training that the Venezuelan migrant
brings and the occupation they perform: of 575
people who completed their university or technical
degree studies, only 7,65% are working in their eld
of study (university students and technicians in their
profession), while 92.35% are working in some other
activity. Among those surveyed, inappropriateness
affects both men and women in a similar proportion.
It should be taken into account that, sometimes,
countries limit the incorporation of workers to certain
occupations or professions, so this inappropriateness
is not always due to barriers related to the recognition
of degrees.
3.4 Lack of decent work and job
precariousness
The majority of Venezuelan migrants and refugees,
regardless of their educational level and work
experience, are working in the informal sector.
The most frequent occupations are: in shops,
street vendors, customer service, restaurants and
construction; a majority of women are relegated
to paid care and domestic work. Informal working
conditions do not meet the requirements of labour
legislation. They are characterized, on the contrary, by
the lack of a written employment contract, existence
of longer or shorter working hours than desired,
payment of minimum wage or less, non-payment
of wages, lack of social protection (they do not have
access to health or pension systems), disrespect
for labour rights (bonus, vacation pay and overtime,
among others) and early dismissals after passing the
trial period.
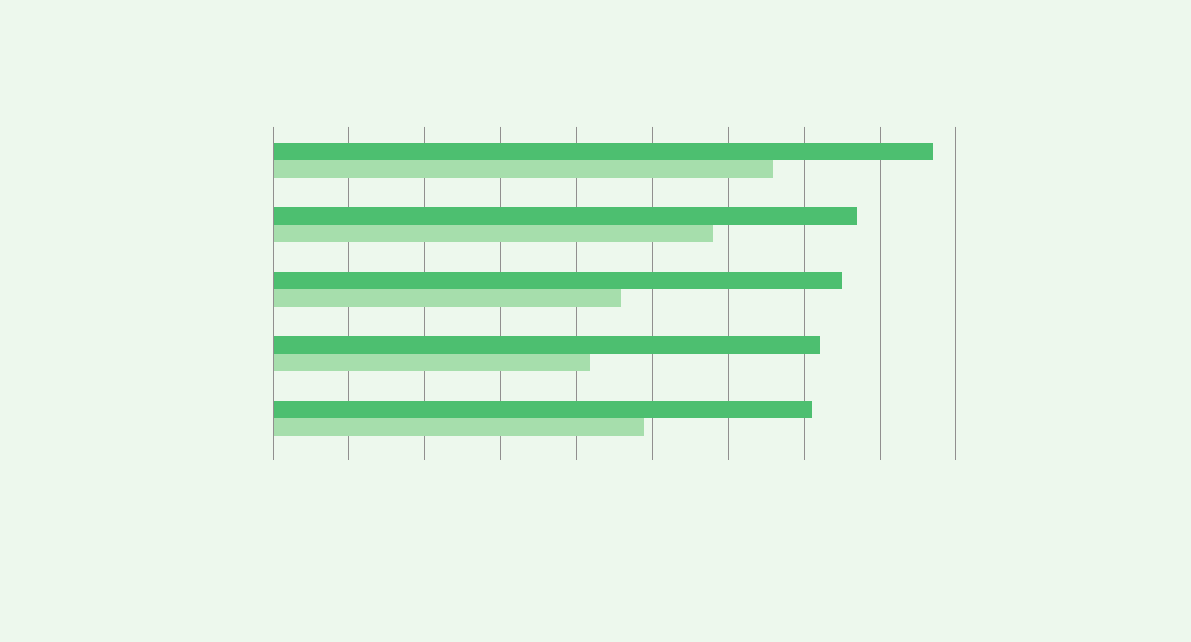
Figure 1 compares the percentages of informal
work among nationals and people of Venezuelan
origin in ve South American countries: Argentina,
28
Migration from Venezuela: opportunities for Latin America and the Caribbean
Brazil, Colombia, Ecuador and Peru. The percentage
of Venezuelans working in the informal sector is
systematically higher than that of nationals and
exceeds 70% in all ve countries. On average, the gap
between the two populations is around 24%.
Graphic 1. Percentage of Venezuelans and nationals in the informal sector, 2018-19
Perú
Colombia
Ecuador
Brasil
Argentina
0 2010
% of Venezuelans working in the informal sector
% of nationals working in the informal sector
30 40 50 60 70 80 90
Source: World Bank (2020).
In Chile, Salgado et al. (2017) report that 45% of the
Venezuelan people surveyed in their study entered
the labour market as salespeople and that another
20% are working as waiters, which is equivalent to
saying that 65% work in the service sector, under the
modality of customer service. In Peru, Tincopa et al.
(2019) point out that 29% of women who work do so
in itinerant or informal jobs and 43% in jobs related
to direct sales or customer service. Thus, “a very
notable characteristic of the Venezuelan migrant
population in all the countries of South America,
including Ecuador, is their presence in the streets,
squares, parks and markets, selling products such as
sweets, fast food, homemade sweets, juices, or the
traditional Venezuelan arepa ”(Ramírez et al., 2019,
p. 20).
Koechlin et al. (2019) note that a visible characteristic
of the labour insertion process consists of “the
precarious working conditions in which a signicant
percentage of immigrants nd themselves. (…) The
precarious factors are reflected in the working hours,
salaries, formality and informality of employment,
job rotation ”(p. 36). The study shows that, for
Lima, Arequipa and Piura, 82% of the Venezuelan
people surveyed reported working longer than the
established legal workday, which is equivalent to 48

Regional socio-economic integration strategy
29
hours per week
10
and 46% reported having an income
below the minimum wage. When introducing the
gender variable, the study nds that more Venezuelan
women receive an income below the minimum
compared to their male peers (58% reported by
women versus 37% reported by men).
For Chile, Salgado et al. (2017) point out that although
49% of the people surveyed had a written contract,
“some 43.1% of those who have a contract, do not
contribute to the pension fund. This situation has a
certain correlation to when they were asked if they
were contributing to the health system (…), 17.4% of
those who have some type of employment contract
do not contribute to the health system ”(p.108). Célleri
(2019), in the study on Ecuador, found that 51% of
the people surveyed with a job have a dependency
relationship, but 70% indicate that they have not
signed a contract. According to the author, a possible
explanation for this situation is that they enter jobs
under the condition of a “probationary period,” which
according to current legislation in Ecuador is three
months, a period in which employers can make
dismissals without the obligations that they would
have under a xed contract and with the payment of
social security.
This situation is also evident in the DTM reports.
In Brazil, 80% of the people who reported being
employed receive less than the minimum wage and
72% did not sign any employment contract (DTM
April 2019). In Paraguay, 20% of the people who
reported employment earn less than the minimum
wage (DTM October 2018). In Trinidad and Tobago,
47% of Venezuelan people who work reported earning
less than the minimum wage and 23% reported
being in violation of their labour rights for not being
paid or being paid less than the agreed salary (DTM
September 2018).
10 When cross-analyzing the variables of working hours and remuneration, the study found no relationship between greater number of
hours worked and higher remuneration.
Women also face the worst working conditions in
the informal sector; more often they lack a contract,
earn less than the minimum and less than their male
counterparts (wage gap), and work fewer hours than
desired. They also face particular risk situations at
work or when searching for work: sexual harassment,
abuse and rape. They are, therefore, subject to dual
employment discrimination due to their status as
women and refugees or migrants.
Pressure is evident in the labour market due to
informal, low productivity and precarious jobs.
There is an oversupply of labour for this type of
work, which results, on the one hand, in an increase
in job insecurity, which affects both nationals and
refugees and migrants and, on the other, an increase
in xenophobia and discrimination.
3.5 Impact on employment and
work due to the measures
adopted to stop the spread
of COVID-19
The COVID-19 pandemic triggered a veritable health,
socioeconomic and care crisis. The quarantines
and other physical distancing measures adopted to
prevent the spread of the virus, although necessary,
generated an economic recession at the global
level that resulted in a decrease or paralysis of
productive activities, especially in sectors such as
hotels, construction, restaurants, travel and tourism;
a strong increase in unemployment and a reduction
in working hours and income (UN, 2020). The
International Monetary Fund (IMF) projects that real
GDP will suffer a drop of 3% in the world in 2020 and
a drop of 5.2% in LAC (IMF, 2020). The UNDP (2020a)
anticipates that the Human Development Index (HDI)
could reverse for the rst time in three decades.

30
Migration from Venezuela: opportunities for Latin America and the Caribbean
Recent ILO estimates show a decrease in the number
of working hours of around 10.7% compared to the
last quarter of 2019, which is equivalent to some 305
million full-time jobs in the world (based on a 48-hour
workweek) and a reduction of 13% in the Americas
(ILO, 2020a). These same estimates show that many
young people under 30 years of age, who make up
around 70% of international migratory flows at the
international level (ILO, 2017b), were affected by the
closure of work centres and borders. The productive
sectors that are most affected are precisely those
with the greatest presence of young workers (ILO,
2020a).
In the world, almost 1.6 billion workers in the informal
economy were affected by isolation measures or
by working in the most affected sectors, and their
income was reduced by 60% during the rst month of
the crisis (ILO, 2020). According to the Inter-American
Development Bank (2020), the level of informality
could reach 62% in Latin America and the Caribbean,
a percentage that currently stands at 54%, according
to the ILO.
In 2020, the poverty rate could increase to 4.4% and
the extreme poverty rate to 2.6% compared to 2019,
reaching 34.7% of the Latin American population
- which is equivalent to 214.7 million people -; for
its part, extreme poverty would reach 13% - which
is equivalent to 83.4 million people (ECLAC, 2020d,
cited by ECLAC and ILO, 2020).
People who work in the informal economy and who
are therefore not covered by the countries’ social
protection systems are the ones who are most
affected by the economic and labour crisis. Refugees
and migrants, who also suffer the consequences
of xenophobia and discrimination, constitute a
particularly vulnerable population because most
of them work in activities related to commerce and
services, including itinerant sales, domestic work,
11 “Interagency Group on Mixed Migration Flows,” Colombia, which is part of the Coordination Platform for Refugees and Migrants from
Venezuela, R4V.
caring for children and the elderly, construction and
recycling, all informally (UNDP, 2020b). As expected,
these activities will be among the most affected when
the restrictive measures adopted due to the health
crisis are totally or partially lifted. The economic
reactivation process will also depend on the
conditions in which the companies nd themselves
in order to operate again. Many had to close, lay
off staff or slow down their production, so they did
not receive or perhaps do not receive support from
governments (tax benets, extensions to pay debts,
subsidies to keep jobs, reduction of social costs, etc.)
and will have serious difculties in resuming their
activities.
Since there is not yet a vaccine, the population will
have to live with the SARS-COV-2 virus and that will
imply an adaptation of the operating rules of many of
the services in which the migrant population is or was
employed, and this will be reflected in the quantity
and quality of jobs. Health and safety regulations
at work are especially relevant in this case, and also
require adaptation to prevent the spread of the virus.
A rapid needs assessment in the context of COVID-19,
carried out in Colombia (May 2020) by GIFMM
11
,
indicates that, since preventive measures were
implemented, 20% of households report receiving
income from paid work when before, this number
was up to 98%, which shows a decrease of 78%.
In addition, 48% of the people surveyed said they
did not have any source of income, which implies
a signicant increase compared to the 4% who
reported no income before the isolation measures.
Also noteworthy is the increase in the percentage of
households that are using their savings (before, they
were used by 2% and now, by 13%).
Those who work in activities such as, for example,
the distribution of food - with a strong presence of
Venezuelan workers - did not suffer restrictions on
Regional socio-economic integration strategy
31
mobility because they are “essential services,” so they
can continue to function despite the social distancing
measures. However, they were exposed to the risk
of contagion because they lacked, in all cases, the
necessary protective elements and were not covered
by social protection, in addition to encountering
difculties in joining workers’ organizations and
establishing dialogues with the employment sector.
School closures and, in many cases, distance
learning can put a strain on families; in particular, for
women, who dedicate three times as much time to
unpaid care and domestic work as men. Furthermore,
gender inequalities are accentuated in households
with lower incomes, in which the demand for care
is higher, given that they have a higher number of
dependents per household (ECLAC, 2020a).
Finally, the massive arrival of the population from
Venezuela made it difcult to design a response to
the demand for housing. This additional vulnerability
factor was increased by the context of the COVID-19
epidemic. In fact, the excluded neighbourhoods,
which have an overrepresentation of the refugee
and migrant population, are particularly affected,
given that the shelters, short-stay hotels or shared
apartments are highly overcrowded spaces with poor
infrastructure, which represents a vehicle for the
spread of the virus and an increased risk of exclusion.
3.6 Social protection in the
regional context
Social protection, which includes social security, is a
human right that is dened as a set of policies and
programs designed to reduce and prevent poverty,
vulnerability and social exclusion throughout the life
cycle. The provisions of Convention No. 102 of the ILO
on the minimum standard of social security (1961)
establishes nine main areas of protection: family
and child benets; maternity and unemployment
benets; benets in case of accidents at work and
occupational diseases; sickness, old-age, disability
and survivors benets, and health protection. The
provision of all these benets is made through a
combination of contributory schemes based on
traditional social insurance and non-contributory
benets nanced by taxes (ILO, 2017a).
Beyond recent advances in the consolidation of
comprehensive social protection systems in Latin
America and the Caribbean, signicant coverage
gaps persist in geographical terms (with marked
differences between urban and rural areas) and
especially with respect to some groups considered
difcult to cover, as in the case of migrant workers
and their families. The countries developed their
social protection systems on the basis of different
starting lines and various institutional schemes
and, therefore, the results achieved are quite
heterogeneous in terms of coverage and quality of
benets. Currently, more than ve out of ten workers
do not contribute regularly to social security and,
therefore, lack any type of coverage.
Colombia promoted, through the Special Residency
Permit (PEP), the regularization of the Venezuelan
population, to facilitate their access to formal
employment. Thus, the immigration authorities
regularized more than 660,000 Venezuelans in
less than three years. However, coverage rates for
Venezuelans in a regular situation within the social
protection system remain relatively low. As of April
30, 2020, the number of PEP holders registered in the
Single Database of Afliates (BDUA) of the General
System of Social Security in Health was 216,285, that
is, only 32.7% of Venezuelans are PEP holders (UNDP
/ Presidency of the Republic of Colombia, 2019).
In addition to traditional problems such as high
informality, there are other elements that exert pressure
on the performance of social security systems, such
as accelerated technological change and disruptions
in the organization of production and work; the aging
of the population and the increase in dependency
rates; the incidence of natural disasters and, also,
the phenomenon of labour migration (ILO, 2018).

32
Migration from Venezuela: opportunities for Latin America and the Caribbean
A global mapping conducted by UNHCR in 2018
found that most national social security systems are
not accessible to non-nationals. In the few countries
where access is given to refugees, it is partial or
limited due to restrictive legal frameworks or barriers
to implementation
12
. Over the years, an understanding
has been achieved on the part of both the authorities
and the general population that these programs do
not depend on the discretion of the government in
power, but rather are rights that must be guaranteed
by the States (ECLAC, 2017). Non-contributory
social protection policies were implemented through
the appropriate institutions using available public
funds and with a commitment to implement them
from a human rights perspective. In addition, these
policies have an international, constitutional and
legal framework which recognizes the right to social
security of all people without distinction.
All these factors mean that the region has a
favourable framework for promoting the inclusion of
refugees and migrants in national social protection
systems
13
.
Due to the serious situation in the LAC region resulting
from the effects of the pandemic, governments
applied different measures to extend social
protection to the populations in which COVID-19
caused the greatest damage. At the beginning of the
pandemic, the use and adaptation of existing cash
transfer programs was the most frequent response.
Due to the prolongation of the health crisis and the
limited coverage of social protection instruments,
which were not enough to cover vulnerable
populations such as informal workers and vulnerable
households, new instruments such as vouchers
12 Phelps, Laura: Mapping opportunities for linking humanitarian cash-based interventions with national social safety nets for displaced
populations, UNHCR, March 2018.
13 “The incorporation of refugees in national non-contributory social protection programs (social assistance) in the Americas, how to
move forward?” UNHCR July 2018.
14 https://www.ilo.org/global/about-the-ilo/newsroom/news/WCMS_633165/lang--es/index.htm
15 United Nations Development Programme (2020). Technical Note: the economic impacts of covid-19 and gender inequalities
recommendations and guidelines for public policies. Retrieved from: http://americalatinagenera.org/newsite//images/cdr-
documents/2020/04/PNUD_GENERO_COVID19__ESP_FINAL_ok_5.pdf
and transfer programs were created. However, the
migrant population was not always included in these
responses (Rubio, Escaroz, Machado, Palomo and
Sato, 2020).
COVID-19 response measures such as isolation
highlighted the global care crisis and, in particular,
global care chains
14
. Within the framework of social
protection, care must be understood as a basic right
of citizenship that the community assumes and
guarantees in order to maximize individual and social
well-being, with direct supervision of the State in the
provision of care services and the regulation of the
responsibilities assumed by other institutions.
Unpaid care and domestic work increased as a
result of the COVID-19 outbreak, from caring for
patients at home and the elderly, school closures
and mandatory quarantines. Women and girls are
the primary caregivers in the home and have greater
domestic and family care responsibilities. Worldwide,
they do two and a half times more unpaid care and
domestic work than men.
Migrant women, especially those who are involved in
domestic care, face a greater possibility of exposure
when they maintain their economic activity and when
they are unable to do so, as a consequence of travel
and mobility restrictions, they experience harsh
socioeconomic consequences derived from income
losses. Unequal power relations and discriminatory
social norms can pose additional risks for migrants in
contexts where discrimination and xenophobia limit
their access to a source of employment, livelihoods
or services
15
.

Regional socio-economic integration strategy
33
4
Priority axes of the
regional strategy
for socioeconomic
integration
The Regional strategy for socio-economic integration aims to respond to
the needs of this population not only with humanitarian actions, but also
with measures aimed at their socio-economic integration. In this sense,
the Strategy is part of a medium- and long-term framework and recognizes
that the majority of refugees and migrants from Venezuela will settle for
many years, which is why the only viable option for them to contribute to the
Sustainable development of their host countries is to promote socio-economic
integration and citizen coexistence. With this objective, the Regional Strategy
focuses on seven axes: (i) Regularization and proling of the population from
Venezuela; (ii) Professional training and recognition of degrees and skills; (iii)
Promotion of employment; (iv) Entrepreneurship and business development; (v)
Financial inclusion; (vi) Access to social protection, (vii) Social cohesion.

34
Migration from Venezuela: opportunities for Latin America and the Caribbean
4.1 Regularization and proling
of the population from
Venezuela
The regularization of migration and the recognition of
refugee status are central elements of the integration
of refugees and migrants into their host countries.
Having the necessary documentation is essential
for them to have access to services and the formal
job market. However, in many Latin American and
Caribbean countries, a large proportion of the
Venezuelan population is in a situation of irregular
stay. For some people, this is because they used
irregular channels to cross borders or because they
do not have ofcial documentation, which is difcult
to acquire in Venezuela; for others, it is because
they encountered legal or practical barriers to
accessing refugee status determination procedures,
and the rest, because the host countries increased
restrictions on regularization. Faced with this, public
authorities in the region should adopt more flexible
and expeditious regularization mechanisms, as
well as improve their asylum systems to favour the
integration of migrants and refugees and increase
their contribution to the economies and societies of
the countries receiving them.
On the other hand, as a complement to the
regularization processes, it is important to have
detailed data on the socio-labour proles of the
Venezuelan population, as well as the returnees, to
better understand who they are and what their areas
of training and experience are, and thus seek a better
insertion into the labour markets of the host countries.
On the other hand, to favour the matching process
between demand and labour supply, information is
also needed about the characteristics of the labour
demand.
u Current situation / obstacles
An important part of the Venezuelan population is
in an irregular situation in many countries of the
region.
In many countries, the Venezuelan population,
particularly the most vulnerable, has limited
access to the information available on the
different options for regularization.
The regularization mechanisms that were
implemented in most of the countries of the
region are relatively rigid and prevent addressing
the permanent flow of people from Venezuela.
The high costs of visas and the long periods
needed to respond to the procedures represent
another obstacle to regularization.
Despite the fact that many Venezuelan nationals
could qualify as refugees, few are ever recognized
as such by the authorities of the host countries.
Some of those who returned do not have
the necessary documentation to prove their
nationality and are in an irregular situation.
Efforts to characterize the refugee and migrant
population remain very limited.
There is a scarcity of data on the population from
Venezuela disaggregated by sex, diversity, age,
ethnic origin, and disability status, among others.
Detailed and systematic data is lacking on the
educational and socioeconomic characteristics
of the population from Venezuela and their ability
to enter the labour markets.
When they exist, a systematization of the data
about the characteristics of the labour demand is
required.
There is a lack of knowledge on the part of the
private sector regarding the validity of the regular
stay documents and about the processes for
hiring refugees and migrants.

Regional socio-economic integration strategy
35
u Proposal
In order to address the massive arrival of refugees and
migrants from Venezuela and facilitate their process
of socio-economic integration, it is necessary for the
governments of the recipient countries to implement
processes of regularization of the Venezuelan
population in an irregular situation, recognition
of their refugee status through the persons who
qualify and requested protection, and proling of
the returned population (including persons born in
Venezuela who are the sons and daughters of Latin
American refugees and migrants).
Such regularization and proling processes, which
are based on a registry of the population from
Venezuela, as Colombia did in recent years through its
Special Stay Permits (PEP), are the most effective in
allowing refugees and other migrants to successfully
enter formal labour markets and contribute to the
economic growth of their host countries (Clemens,
Huang, and Graham, 2018). In this sense, one of the
rounds of PEP in Colombia covered people who had
entered the country irregularly as long as they had
registered with the government between April and
June of 2018, which allowed for the regularization
of large numbers of Venezuelans. Argentina and
Uruguay, for their part, grant MERCOSUR residence
visas to people from Venezuela, despite the fact
that this country was suspended from this body.
In the rst case, they obtain a temporary two-year
visa. In the second, a permanent resident visa. Upon
entering, Brazil grants temporary residence to any
Venezuelan person as long as they have some type
of identity document, which allows them to arrange
for permanent residence three months before the
previous one expires, although they must prove that
they have a legal source of income. Peru, through
the Temporary Permit of Permanence (PTP), allowed
people to move to a migratory category of long-term
16 This measure follows the decision, adopted in June 2019 by CONARE, to recognize that the situation in Venezuela constitutes a serious
and widespread violation of human rights, as described in the Cartagena Declaration on Refugees of 1984.
residence after one year, but at present, the program
is closed (Selee and Bolter, 2020).
Some examples of migrant registries are: Colombia,
with the Administrative Registry of Venezuelan
Migrants (RAMV), which collected information on the
size and prole of this population, specically those
who were in an irregular situation, as it was carried
out during the round of PEP for people in irregular
condition; and Ecuador, started in September 2019,
which provides information on an approximate
number of migrants from Venezuela, their
characteristics, migratory situation, socioeconomic
position, and work and educational proles (Selee
and Bolter, 2020).
Another important example of regularization was the
decision of the Brazilian government to recognize the
refugee status of Venezuelans through group-based
determinations, such as the prima facie approach.
Under this approach, asylum applications that
meet the necessary criteria are processed through
an expedited procedure, without the need for an
interview
16
.
It is necessary to make procedures more flexible
and to extend the criteria for recognizing refugee
status, so that the Venezuelan population benets
from greater protection and the processes of
socioeconomic integration in the host country are
accelerated. Several countries in the region extended
the denition of “refugees” in their national legislation
based on the Cartagena Declaration on Refugees -
as is the case of Brazil (UNHCR, 2019) -, while others
increased their capacities to process applications
for asylum or developed simplied or accelerated
processes.
It is also important to carry out proling processes
for the migrant population from Venezuela, which
include refugees, asylum seekers and returnees,

36
Migration from Venezuela: opportunities for Latin America and the Caribbean
through coordinated surveys among the different
entities in charge of providing care in different
areas and those that participate in the process of
socioeconomic integration, in particular the Ministries
of Labour, Education, Health and Social Protection,
as well as the departments of statistics. The proling
processes must consider that, many times, the
reasons for leaving Venezuela are associated with
the criteria for recognition of the refugee’s condition,
such as persecution, situations of violence or serious
disturbances of public order that threaten the life, as
well as the security or freedom of these people.
u Strategic lines
1. Adoption of flexible regularization mechanisms
Adopt different migratory categories or create
ad hoc temporary alternatives (for example,
special residence permits or humanitarian
visas), to enable access to services and
insertion into formal labour markets.
Strengthen national asylum capacities,
including improving refugee status recognition
processes to reduce response times and make
conditions more flexible, so that a greater
number of asylum seekers can access the
refugee qualication and, therefore, obtain
recognition of their legal status.
Improve the information and guidance
mechanisms for the regularization processes
of Venezuelans, aimed at employers, and both
employers’ and workers’ organizations.
Reduce the costs of visas and residence
permits, when they have a cost, or apply
special rates for vulnerable populations.
Create regularization mechanisms for people
in an irregular situation who obtain a formal
employment contract.
In the context of COVID-19, adopt more flexible
regularization mechanisms to guarantee
greater protection, which simplies the
incorporation of migrants and refugees into
the labour market in a context where the need
for foreign labour was more than evident.
2. Streamline the proling processes of the
returned population from Venezuela
Information and orientation mechanisms so
that people who return to Venezuela after
several years or even decades know their rights
and the current processes for the recognition
of their nationality in their country of origin.
Facilitate proling processes so that returnees
and, in particular, those belonging to the
“second generation” can request recognition
of nationality in their country of origin (or that
of their parents).
3. Proling of the demographic and
socioeconomic prole of the population from
Venezuela
Collect existing information to avoid
duplication of efforts / studies and waste of
resources.
Carry out studies that assess the living
conditions of the population from Venezuela
such as: the composition of the household;
access to health, education and childcare
services; level of education and professional
skills; work and business experience, as
well as vocational prole; current economic
activity and working conditions; cases of
vulnerability, discrimination and labour
exploitation; the situation of migrant women
and the specic obstacles they face; ethnic
minorities: indigenous and Afro-descendant
communities.

Regional socio-economic integration strategy
37
4.2 Professional training and
recognition of degrees and
skills
Investing in vocational training is a key aspect of
the process of socio-economic integration since it
reduces the gap between the demand and supply
of skills. While it is true that a part of the population
from Venezuela is educated and has skills that
can be useful for the economies of the countries
of the region, another part requires technical or
complementary training, including socio-emotional
skills, to better meet the needs of labour markets
in the host countries and thus facilitate their job
placement. In this sense, it is important to involve
employers’ and workers’ organizations in the design
of vocational training programs so that they consider
the needs of companies.
Another essential stage in the labour inclusion
process is the validation of technical and academic
qualications, so that studies completed outside the
destination country are recognized. This validation
process, although not a legal requirement in all
sectors, opens up more formal employment options.
But in practice, there are many obstacles that
make it difcult or prevent most professionals from
validating their qualications, so they nd themselves
in a precarious employment situation despite their
academic level.
For their part, in many countries, people without
degrees but with professional experience have the
option of requesting recognition of this experience
through skills certication mechanisms. Recognition
of previous learning acquired throughout working
life can facilitate the process of insertion into the
job market for the Venezuelan refugee and migrant
population, as well as for returnees.
u Current situation / obstacles
The channels of communication and coordination
between public employment services, companies
and vocational and technical training institutes
need to be streamlined and strengthened so that
the training offered is relevant and meets the
needs of the job market.
The incorporation of women continues to be
widespread in areas or occupations traditionally
assigned by gender. Afrmative measures are
required for the promotion of gender equality.
Most of the people from Venezuela are inserted
in occupations that are not related to the studies
they have completed.
The underutilization and waste of their job skills
represents a loss not only for the refugee and
migrant population, but also for the national
economy that is deprived of skills and capacities
that it might need.
In many cases, qualied persons, whether
Venezuelan or returnees, do not carry their
diplomas acquired abroad.
They face difcult requirements to full, such
as the apostille of certicates and technical and
academic degrees in Venezuela or, in certain
cases, their translation.
They must assume high costs and long
procedures to validate degrees that account for
the studies obtained and thus certify their skills,
acquired formally or informally, which means that
they must be underemployed and self-employed
in the informal sector.
Women are the ones with the highest levels of
imbalance, since they have the highest levels of
education (as a group), but also the highest levels
of underemployment.
In many countries, refugees and migrants in an
irregular situation are unable to validate their
qualications or certify their skills.

38
Migration from Venezuela: opportunities for Latin America and the Caribbean
u Proposal
The denition of the training curricula must be aligned
with the requirements of the companies, market
studies and information collected by the public
employment services and duly accredited private
employment agencies. Due to the impact of the
pandemic, the new dynamics developed around work
promoted the construction and operation of digital
platforms to promote the sale of goods and services,
and thus enable communication between very
diverse actors from different geographical locations.
At this time, training institutes have an opportunity to
capture these possibilities and transform them into
new careers or enrich / adapt existing ones, including
those in health-related areas.
The wastage of the competencies of migrant
workers is caused by difculties in the recognition
of prior learning (RPL), which, in turn, is due to
difcult-to-meet requirements established by
the responsible institutions. They have to do with
costs, misinformation, duration and immigration
documentation, among others, which are related to
legal or regulatory provisions that would need to be
reviewed to enable more inclusive access. The RPL
also nds limitations because some countries may
not recognize certain competencies, a barrier that
could be reversed at a regional level, working on
frameworks that homogenize the qualication.
In other cases, the limitation originates from the
lack of studies that determine which skills the
market needs to have strengthened or developed,
and the consequent training offer, which must
also be reviewed and updated. The participation
of representatives of workers and employers is a
conducive channel for identifying the necessary and
17 Emergency Decree No. 037-202. El Peruano (Sunday, April 12, 2020): https://www.mef.gob.pe/es/normatividad-sp-9867/por-
instrumento/decretos-de-urgencia/22200-decreto-de-urgencia-n-037-2020-1/le
18 Ofcial Decree 260 (Thursday, March 12, 2020). Ofcial Gazette of the Republic of Argentina No. 34.324: https://www.boletinocial.gob.
ar/suplementos/2020031201NS.pdf
available skills, which opens the possibility of working
on the gaps (OECD / UNHCR, 2018).
Some countries facilitate the process of validation
of degrees by making the procedure free, as is the
case of Argentina, Ecuador and Uruguay. Argentina,
in February of 2018, began to recognize the degrees
as if there was a reciprocity agreement between the
two countries, even though it does not exist, which
eliminated the apostille requirement and accelerated
their management by decentralizing the validation at
different public universities in each of its provinces.
Uruguay had a centralized system in a university in
the country and, with the increase in immigration,
it decentralized the procedure in different university
faculties, which reduced waiting time (Selee and
Belter, 2020).
The response to the COVID-19 pandemic highlighted
the need to recruit refugees and migrants to meet
the demand for local labour, particularly in the health
and care sectors. In this sense, some countries
accelerated and simplied the procedures for
validating the qualications of health professionals
in order to increase the number of personnel
assigned to care for infected people. Peru ordered
the hiring of refugees and migrants who were
medical professionals to reinforce health care in
the face of the COVID-19 emergency. To do this, it
created the Special COVID-SERVICER Service, made
up of medical professionals, to exclusively attend to
the health emergency and in which both Peruvian
health professionals, refugees and migrants
17
can participate. In Argentina, by means of Ofcial
Decree 260 of Thursday, March 12, 2020, authorized
“exceptionally and temporarily the hiring and exercise
of professionals and health technicians graduated
abroad, whose degree is not revalidated or enabled
in the Republic of Argentina
18
. “These measures

Regional socio-economic integration strategy
39
could have continuity and, at the same time, are an
example of good practices that may be replicated in
the future in light of the needs of the labour market in
other areas or occupations.
u Strategic lines
1. Vocational training
Review of admission requirements for the
refugee and migrant population at training
institutions for work.
Development of training courses in the sectors
of the economy and branches of economic
activity with the greatest demand in the
market, in consultation with employers’ and
workers’ organizations.
Promotion of careers in information and
communication technologies, as well as in the
provision of cleaning and disinfection services
in health establishments, management of
elements of risk to biosafety in occupational
spaces, risk and health management systems
and security against COVID-19, among others.
Strengthening the link between vocational
training and public employment services,
as well as with workers’ and employers’
organizations, so that there are feedback
channels about the occupations in greatest
demand, capturing the needs of companies
and referring the seekers of employment to
vocational training institutes.
Construction, in association with organizations
and bodies that are working in this area, of a
regional occupational framework to facilitate
labour mobility.
Promotion and facilitation of women’s access
to technical and professional training on equal
terms with men and in non-traditional areas.
Consolidation, through social dialogue, of the
link and congruence between employment,
qualications and migration policies, which
generates an exchange of information between
the educational system and the labour market,
in order to develop training procedures in
relevant elds and anticipate the needs.
Construction, through tripartite dialogue, of
training modalities that include training in the
workplace.
2. Validation of degrees granted in Venezuela
Adopt a flexible process for the validation of
degrees obtained abroad and reduce costs,
especially in the context of COVID-19.
Creation of a fund to subsidize the process of
validating the degrees of the most vulnerable
people.
Design of alternative mechanisms to the
apostille, to be able to recognize the degrees
granted abroad.
3. Competency certication
Increase in nancial and human resources at
the disposal of the competency certication
bodies, to streamline the certication
processes.
Mapping of public employment services and
the degree of attention to the refugee and
migrant population, as well as referral to
training or recognition of prior learning (RPL).
Review and simplication of procedures and
requirements for RPL, as well as associated
costs, especially in the current context of
COVID-19, which demonstrates the need to
incorporate more of the Venezuelan population
into the job market.

40
Migration from Venezuela: opportunities for Latin America and the Caribbean
Prospective employment studies for
professional updating or reconversion.
Holding meetings with representatives
of employers and workers, analysis with
employment platform rms and review of
successful insertion practices, as well as
aspects to improve.
4.3 Promotion of employment
Economies in the region are characterized by
high levels of informality, unemployment and job
vulnerability. The migrant population, particularly
the female population, is particularly exposed to this
vulnerability. The lack of economic opportunities
causes many people from Venezuela to look for
options in the informal sector, but also, in some cases,
to resort to illegal activities that can contribute to
increased citizen insecurity in the host communities.
In this sense, the best humanitarian aid that public
authorities can provide is to facilitate the access
of the refugee and migrant population to labour
markets.
The Colombian Special Residency Permit for the
Promotion of Formalization (PEPFF) allows the
regularization of Venezuelans who are in an irregular
situation, provided they have received an offer of
formal employment. In Brazil, Costa Rica and Peru,
those seeking asylum are granted a temporary work
permit, so they can remain in regular immigration
status while their case is resolved (Selee and Belter,
2020).
u Current situation / obstacles
The labour insertion of refugees and migrants
occurs, above all, in the informal sector of the
economy. Many times, they work as street
vendors and shop assistants.
Most of the region’s labour markets maintain high
informality rates and have difculties absorbing
the demand for labour.
The condition of irregular stay due to the lack
of identity or immigration documents restricts
the possibilities of getting into a decent job and
forces them to work informally.
A large part of this population reports income
below the minimum wage and working hours
greater than 48 hours a week.
Their unionisation rate - in the studies where
it was investigated - is very low. There is great
ignorance about the right to organize and fear of
exercising it.
This population often lacks a written contract.
Migrant women:
Are more affected by unemployment and
underemployment than men, and they receive
lower wages, mostly below the minimum.
Work fewer hours due to the need to care for their
children, and because of the lack or difculty in
accessing these services.
Are more exposed and more affected by
situations of violence and sexual and workplace
harassment.
Are mainly offered customer service jobs
that, deep down, have a sexual connotation of
attractiveness or “hook” to convince potential
clients or consumers (ILO and IOM, 2019), so
there is a bias in the job offer. However, these
prejudices and perceptions also expose them
to situations of sexual exploitation and human
trafcking and limit their access to “traditional”
jobs such as caring for children and the elderly or
housework. They are more likely to be victims of
human trafcking and migrant smuggling.

Regional socio-economic integration strategy
41
u Proposal
Generating the necessary capacities in the Ministries
of Labour is the rst step in designing proposals
that promote employment, particularly the Public
Employment Service and Labour Inspection.
The demand for these services underwent a notable
increase in most of the countries and generated its
necessary modernization through technological
tools that facilitate labour intermediation, such
as, for example, applications and databases that
collect information on occupational and professional
proles. Some of these services may establish
restrictions on the access of refugees and migrants,
mainly linked to the required documentation. They
must be identied, and reform measures must be
taken that may imply modications in administrative
regulations or specic laws. Alliances with the
private sector and workers’ organizations are key
to knowing the requirements of companies and the
availability of labour. The promotion of employment
in rural areas should be incorporated in order not
to restrict job opportunities to the most populated
cities and to supply the workforce that is sometimes
needed in rural areas. Migration can even represent
an opportunity and should be included in the design
of strategies aimed at revitalizing rural areas. Having
a young population that is available to work and often
has higher qualications and skills than nationals
can ll labour shortages not only in agricultural
activities, but also in activities that require more skills
and that, usually, due to their geographic location do
not attract national professionals.
The promotion of women’s employment should also
be incorporated in order to overcome the prevailing
bias towards offering women customer service jobs
or sales that expose them to situations of violence
and harassment. It is necessary to promote equity
in employment because Venezuelan women have
higher educational levels than Venezuelan men,
but they are more affected by unemployment and
underemployment, and they are the ones who receive
a higher percentage of wages below the minimum or
lower wages in comparison with their male peers. At
the same time, it is important to coordinate actions
with the pertinent state agencies to address the
limitations they have in access to work due to the lack
of care services and even access to the educational
system for their children. Also, it must be ensured
that pregnant or lactating women have equal access
to the world of work.
As for Labour Inspection, the vulnerable position in
which many refugees, migrants and returnees nd
themselves promotes the precariousness of their
working conditions and the non-observance of their
rights. A sensitized and trained inspection team which
has the technical and technological tools necessary
to identify work centres with a high concentration of
this population is key to recording and monitoring
the correction of infractions and thus protecting their
rights. The Labour Inspectorate must receive training
on ILO Convention 190 on the elimination of violence
and harassment in the world of work, in order to
contribute to the prevention and elimination of this
type of violence; It must also be empowered and act
if necessary, both in the formal and informal sectors,
whether due to violence committed by employers,
co-workers, clients or suppliers, with special regard
to violence and gender-based harassment.
u Strategic lines
1. Promotion of access to the different programs
and services available for guidance and job
placement
Review of the requirements for access
by refugees and migrants, in particular
those referring to the required immigration
documentation.
Establishment at the local level of alliances
with the private sector, workers’ organizations
42
Migration from Venezuela: opportunities for Latin America and the Caribbean
and local governments, to adapt both the
demand and the supply of employment.
Carrying out studies to characterize the
supply and demand of labour, data collection
and processing (qualications, educational
level, sector where they manage to insert
themselves, number of refugees and migrants
who request services and recruitment of job
offers, among others).
Preparation of studies of manpower needs and
skills for the future, with programs for adapting
skills to projections of future demands, framed
in the future of work and attentive to the
economic reality generated by COVID-19.
Consideration of the particular conditions in
which labour insertion or reintegration takes
place in the face of the risk of contagion
of COVID-19, which demands additional
measures for health and safety at work,
particularly in domestic services and paid care
for people.
Creation of a regional network of public
employment services to facilitate mobility
among refugee and migrant workers.
Design of specic employability routes for
job seekers from Venezuela in the Public
Employment Services.
Sensitisation of the personnel who provide
services related to situations of gender
violence, which constitutes an obstacle for
the effective labour insertion of women and
access to training services.
2. Promotion of employment in rural areas: so that
job placement opportunities are not restricted
to the most populated cities and the shortage
of labour that is sometimes experienced in rural
areas can be addressed.
Carrying out studies of the supply and demand
for labour in rural sectors.
Strengthening / design of temporary /
seasonal employment programs that respect
national and international regulations, as well
as the agreements signed between countries.
Strengthening strategies that reinforce
urban and rural links, especially with regard
to food systems (production, transport and
marketing).
Increase in public programs aimed at the rapid
recovery of livelihoods in rural territories. Food
production activities are essential to guarantee
the food security of host communities, but
they can also be a fundamental element of
local economic stimulation (food markets and
related activities). These programs should
be oriented towards the host and migrant
communities.
Promotion of public programs that promote
the creation of “green jobs.”
Generation / strengthening of dialogue
regarding rural development policies with
government institutions, workers’ and
employers’ organizations and local social
organizations.
Improved regulation of agricultural worker
recruitment activities to ensure fair hiring.
Increase in the creation of non-agricultural
jobs in rural areas.
Regional socio-economic integration strategy
43
Incorporation of health and safety measures
in agricultural and livestock work to protect
working people in particular from COVID-19.
3. Strengthening of labour administration
Carrying out improvements to the computer
platforms of the public employment systems.
Training and development of reference
protocols to other institutions and programs.
Awareness of civil servants about vulnerabilities
and rights violations that increase the risk to
refugees and migrants, including returnees.
Development of protocols that allow the
exchange of vacancies between the various
host countries.
Strengthening the capacities of the Labour
Inspectorate through training and the design
of protocols for the care of the refugee and
migrant population.
Training for the Labour Inspection on
Convention 190 and its Recommendation
206, to act in the prevention and elimination
of violence and harassment in the world of
work. In turn, to provide the Inspection with
the necessary powers to act in the event
of violence and harassment, including the
issuance of orders that require the interruption
of work activity in the case of danger to the life,
health or safety of the workers.
Supervision of compliance with health and
safety regulations at work by the Labour
Inspection, to guarantee the implementation
of protective measures against COVID-19
in all work centres, with special attention to
domestic work that, due to its characteristics,
requires different strategies.
4. Promoting employability
Dissemination of existing services and
programs through employers’ and workers’
organizations, as well as the requirements for
hiring refugees and migrants.
Creation or reinforcement of the courses
offered for the development of socio-emotional
skills for life and leadership, especially for
women, as well as their promotion through
guidance and job placement services.
Promotion and referral to available professional
training programs (also virtual), including
those related to the area of soft skills.
Emphatic promotion of diverse jobs for
women, with the aim of combating the bias
that only offers women jobs in customer
service and sales, thus increasing the equality
of conditions with their male counterparts.
Dissemination of information on the labour
rights of women and men and for the former,
on mechanisms of protection and complaint
in situations of sexual and labour harassment,
as well as those involving rights related to
maternity and breastfeeding.
Strengthen the capacities of trade union
organizations to organize workers and defend
their rights.
Coordination with the institutions responsible
for facilitating women’s access to care
services, to promote their insertion into the
labour market.

44
Migration from Venezuela: opportunities for Latin America and the Caribbean
5. Adoption of measures for the transition from
the informal to the formal economy, based
on the guidelines of the Recommendation on
the transition from the informal to the formal
economy, 2015 (No. 204):
Productivity: creation or strengthening
of business, nancial and technological
development services; development of sectors
and value chains.
Standards: disclosure, training, simplication
of procedures and social dialogue.
Incentives: for accessing the formal sector
and social protection.
Establish simplied or progressive tax regimes,
depending on the level of consolidation of the
business, such as grace periods during the
rst years of operation.
Strengthen the capacities of trade union
organizations to include specic clauses in
collective bargaining in order to extend labour
protection to these workers.
Supervision: promotion of a culture of
compliance, institutional strengthening and
formalization agreements.
4.4 Entrepreneurship and
business development
The creation of businesses represents an alternative
for the Venezuelan and returnee population that has
productive projects or difculties of insertion into the
formal labour market. At present, only a minority of
refugees and migrants arrive with a small amount
of capital that could be used to start this type of
undertaking. But, to scale these initiatives and
expand business options between this population
and the host communities, it is essential to develop
initiatives that allow for the promotion of potential
entrepreneurs or business projects through training
and support, as well as nancing through alliances
between the public and private sectors.
u Current situation / obstacles
Establishing a formal business involves numerous
regulatory and administrative requirements that
are complex for most entrepreneurs in general
and can represent additional obstacles for
refugees and migrants.
Little availability of programs and services
for business advice or for the promotion and
development of enterprises for the refugee and
migrant population.
Restrictions on access to these programs and
services due to their condition of irregular stay.
Barriers to access nancial services and loans
to start or strengthen enterprises related to
documentation: credit history, possession
of assets, unrecognized identity documents,
ignorance of refugees and migrants as potential
clients.
Women have more difculties accessing credit
because, in many cases, they do not have
collateral, something that is complicated by their
status as migrants.
Most of the Venezuelan people are inserted into
informal jobs or create informal enterprises. Many
of them do not qualify as micro-enterprises, but
as subsistence businesses.
The micro-enterprise segment is characterized
by a high rate of failure (in the rst ve years of
existence, 45% in Peru and 53% in Ecuador) due to
environmental factors, lack of market information,
low productivity and innovation, low business
management capacity and lack of access to
nancial services (IDB, 2018). For refugees and
migrants, who face additional challenges, these
rates are likely to be even higher.

Regional socio-economic integration strategy
45
Most of the enterprises created by the population
from Venezuela are born out of immediate need
(in the absence of adequate employment options)
to support the family and not because a concrete
opportunity has presented itself.
It is also common for mothers without care options
or access to school for their children to engage in
productive ventures in order to balance their care
responsibilities with the need to generate income.
Many times, refugee and migrant women are
forced to take their children to work, which takes
place on the street and in the sales sector, for
fear that they will suffer abuse or violence at the
hands of unknown persons with whom they live in
difcult, often overcrowded conditions.
All the above factors mean that the majority of
Venezuelan refugees and migrants’ ventures are
low in productivity and innovation, informal, with
little long-term perspective, and operating in
already saturated markets.
In conclusion, it is important to develop sustainable
companies that create employment under decent
working conditions and are a dynamic factor
in local economies. In turn, this type of work is
important for women (even with their greater care
responsibilities) and their prole, specic needs
and interests must be considered in order to
provide real opportunities.
u Proposal
The potential to develop sustainable businesses is
rarely fully realized. Among the obstacles to business
development are external factors over which
companies have no control, as well as internal factors
related to the skills and knowledge of entrepreneurs.
In the specic context of refugees, migrants and
returnees, the situation is aggravated by a lack of
19 The Conclusions can be accessed at this address: https://www.ilo.org/empent/Publications/WCMS_114235/lang--es/index.htm
knowledge of the market in the host countries, their
policies and regulations, existing programs in public
and private entities to support entrepreneurship
and due to lack of access to a social and business
network (UNCTAD / IOM / UNHCR, 2018).
It seeks to promote a people-based approach to
sustainable companies, which recognizes that,
in the world of work, the social, economic and
environmental spheres interact inseparably. This
approach is promoted by the ILO in accordance
with the Conclusions regarding the promotion
of sustainable enterprises
19
emanating from the
International Labour Conference of June 2007.
The private sector, through business associations
and Chambers of Commerce, can contribute to this
process by providing technical and nancial support
to business projects initiated by refugees and
migrants, as well as vulnerable people from the host
communities.
u Strategic lines
1. Creating a suitable environment for sustainable
companies and effective integration in value
chains
Macro assessment of the environment
conducive to sustainable entrepreneurship
and recommendations for public policies to
support entrepreneurship.
Proling and analysis of the subsectors / value
chains with high potential for entrepreneurship,
both for refugees and migrants from
Venezuela, as well as for the host community,
with special consideration for women who,
due to their care responsibilities, would benet
from a formal job without a xed schedule.

46
Migration from Venezuela: opportunities for Latin America and the Caribbean
Implementation of the Approach for Inclusive
Market Systems (ESMI), which promotes the
development of value chains for access to
employment and entrepreneurship in small
and medium-sized companies in order to
develop holistic livelihood strategies based on
the market.
Proling and implementation of pilot projects
to promote the integration of refugees and
migrants in new and innovative ventures, and
thus avoid displacement.
Establishment of alliances with constituents
(for example, chambers of commerce in
different areas).
Improvement and / or expansion of business
development services that include: technical
assistance and support with procedures and
registration (company creation, invoicing, tax
registration, permits or licenses); taxation;
access to credit and marketing.
Program to promote the quality of the service
of the Business Development services
operators, which use the Start and Improve
your Business (IMESUN), Gender and
Entrepreneurship Together (GET Ahead) and
Our Coop methodologies.
Adaptation of training programs to the reality
of the pandemic, which requires, among other
things, the design of digital platforms and
greater flexibility in training times.
2. Strengthening and preparing refugees and
migrants from Venezuela for their economic
integration through entrepreneurship
Analysis of the skills, experience and particular
knowledge of the population from Venezuela,
with special attention to women.
Training in managerial capacity of individual
or collective ventures, with the IMESUN, GET
Ahead and OUR COOP methodologies.
Awareness of refugees and migrants about
market opportunities, support programs and
nancial and non-nancial services.
4.5 Financial inclusion
A major obstacle to the socioeconomic integration of
the population from Venezuela is the lack of access
to the nancial system. In most of the countries of
the region, it is very difcult to open a bank account
and, even more so, to benet from credit. This lack
of nancial inclusion also represents an obstacle to
accessing formal jobs or creating businesses. For
this reason, it is important that public authorities
in host countries work hand in hand with nancial
institutions to enable access to these services.
u Current situation / obstacles
The Venezuelan population in a regular situation
has very low rates of nancial inclusion compared
to host communities.
Most of the people from Venezuela do not have
any type of nancial service or product with
nancial institutions in their host countries.
There are legal barriers and banking regulations
that limit the possibilities for opening and / or
contracting nancial products and services by the
refugee and migrant population.
Other obstacles to the nancial inclusion of this
population lie in the lack of knowledge of current
regulations on the part of bank branch personnel,
as well as in the perception that this population
presents a high-risk factor.

Regional socio-economic integration strategy
47
u Proposal
Financial inclusion is an essential requirement for
labour and business formalization. For this reason,
it is important to work hand in hand with nancial
institutions, to sensitise the different banks and their
branches about the rights of the migrant population
in terms of access to the nancial sector, adapt
the offer of services to their needs and make the
mechanisms for access to credit more flexible. On
the other hand, promoting this type of inclusion
implies investing in nancial education programs
aimed at the Venezuelan and returnee population.
Financial institutions have to see this population
as presenting an opportunity to generate new
businesses that can become a source of prots.
Greater access to credit mechanisms is also a way
for Venezuelans to consume and invest more in their
host countries, thus stimulating GDP growth.
With government support, suitable interventions
could be designed to pool public and private funding
in order to partially transfer the risk to Development
Finance Institutions and donors (co-investment,
provision of technical assistance, nancing of market
studies, creation of collateral).
Likewise, the nancial inclusion of the Venezuelan
population can be facilitated by fostering cooperation
between nancial institutions in the region. This
implies, for example, promoting alliances with
banking institutions to develop mechanisms for
shared credit history at the regional level. It could
also be connected with credit bureaus to enable
options for access to commercial banking resources
or consider the possibility of creating regional
guarantee funds so that the Venezuelan population
can benet from loans.
u Strategic lines
1. Facilitate the access of the Venezuelan
population to nancial services
Elimination of regulatory and administrative
barriers that prevent the Venezuelan
population, particularly those in a regular
situation, from accessing nancial services in
their host countries.
Sensitisation of nancial institutions on the
rights of the Venezuelan population through
the development of training programs on
serving refugee and migrant clients, with a
special focus on the situation of women.
Dissemination of information bulletins that
explain the rights of refugees and migrants
and encourage the different actors in the
sector to promote banking among those who
are in a regular situation.
Organization of awareness and training
workshops in municipalities with a high
concentration of population from Venezuela,
so that bank branch personnel are familiar
with immigration issues.
2. Promote nancial education
Formulation and implementation of an
ambitious nancial education plan aimed at
Venezuelans and returnees with modules
specically designed for a population that is
not familiar with the nancial system of the
host / return countries.
In communities where it is necessary, include
host communities in the nancial education
program.

48
Migration from Venezuela: opportunities for Latin America and the Caribbean
Holding nancial education workshops in the
main receiving cities, as well as in areas with
a high migration density, in collaboration with
the different centres for attention to migrants
and the main associations of Venezuelans and
returnees. This is particularly relevant in the
current context of restricted mobility, during
which greater access to digital platforms has
been promoted.
3. Adapt the banking and credit offer to the needs
of the refugee and migrant population from
Venezuela
Mapping of current nancial and non-nancial
services for refugees and migrants, with
special attention to the services provided to
women, as well as an analysis of the quality of
the services.
Design of nancial products adapted to the
specicities of the population from Venezuela,
especially in the current circumstances where,
due to the economic crisis, they have been
more vulnerable.
Development of institutional, nancial and
technical sustainability plans for operators of
nancial and non-nancial services.
Creation of a guarantee fund to facilitate
access to credit for this population and allow
banks to recover a part of their losses in cases
of non-repayment.
Collaboration with key international nancial
institutions, as well as key donors interested
in the self-reliance of refugees and migrants,
to nd blended nancial solutions that could
incentivize nancial service providers to serve
this population.
4.6 Access to social protection
People from Venezuela are characterized by high
levels of vulnerability, difculties in accessing social
security and a predominantly informal job placement.
This situation conspires against effective access to
social protection, resulting in a low or limited level
of coverage. In this context, people from Venezuela
access jobs of poorer quality and low salaries, they
lack social protection against the different social
contingencies to which they are exposed, such as
old age, disability, death, health and accidents from
work, and they do not have safe work environments.
On the other hand, those who achieve formal labour
insertion have all of these coverages and, in addition,
in some cases they can accrue the contribution
periods in each of the national systems to which
they have contributed, thanks to the application of
bilateral agreements and multilateral social security
services (ILO, 2018).
In the current COVID-19 crisis, in low- and middle-
income countries, those who are most affected are
those who work in the informal sector, as well as
people with limited access to health services and
social protection. They are the ones who are most
at risk of falling into poverty and facing greater
difculties in the recovery phase (ILO, April 7, 2020).
These same circumstances of lack of income and
social protection are what lead many people to return
to Venezuela.
u Current situation / obstacles
There is ignorance about the rights to social
protection of the refugee and migrant population,
as well as about all the programs and services
in social protection, both contributory and non-
contributory. In general, the lack of information
that contributes to effective access to social
protection including social security predominates.

Regional socio-economic integration strategy
49
There is poor coverage in terms of non-
contributory social protection programs that
must ensure a minimum level of protection, both
for host communities and refugees and migrants.
Difculties persist in accessing a social protection
floor that guarantees income security throughout
the life cycle and access to essential health
services for the refugee and migrant population,
due to the lack of regular stay documents or other
restrictive requirements.
Mainly informal labour insertion, which prevents
the materialization of labour rights and social
security.
The most recent migratory waves account for
young, pregnant women, those with young
children, and many breastfeeding women. It is
essential to give them and their children access
to health services and food supplements if
necessary, among others.
u Proposal
Recommendation No. 202 of the ILO on national
social protection floors is an important instrument
for closing social protection gaps in countries and,
in particular, those related to refugees and migrants.
The Recommendation species guidelines to
advance in the consolidation of a comprehensive
social protection system, where a social protection
floor plays an important role in guaranteeing both
income security throughout the life cycle and
essential health care. The ultimate objective of this
international instrument is to guide the formulation
of a proposal for the expansion of social security in
coordination with the rest of the social, economic
and employment policies, in order to help guarantee
income security throughout the entire life cycle and
access to essential health services.
The proposal is made up of a horizontal dimension that
refers to the number of people covered and another,
vertical dimension, that refers to the social risks
covered by the system and the level (quality) of both
nancial and in-kind benets. The social protection
floor guarantees a minimum level of security
represented by effective access to income security
throughout the life cycle (children and adolescents;
active ages; and older adults) and essential health
care. Then, it simulates a social protection ladder
that can be climbed to the highest levels, in line with
other international instruments, such as Convention
No. 102 of the ILO on the minimum standard of social
security and those considered third generation, which
stipulate an even higher protection threshold. The
options for implementing a social protection floor
are multiple, and it is possible that contributory, non-
contributory, universal, assistance and / or mixed
regimes may coexist, as well as a combination of all
the above.
The Recommendation establishes that when
designing and putting the national social protection
floors into practice, the Member States must
promote productive economic activity and formal
employment, including the adoption of labour market
policies and tax incentives, policies to promote
education, vocational training, productive skills
and employability, as well as entrepreneurship and
sustainable companies in a decent work framework,
as proposed by this Regional Strategy, while
guaranteeing coordination among all of them. All of
this will help to consolidate a social protection floor
and promote higher levels of social protection for all
people, including the migrant population.
In rural areas, special attention must be paid to
strengthening public non-contributory social
protection programs such as, for example,
conditional cash transfer programs that exist in
all the countries of the region and are aimed at the
poorest populations. These programs should expand
their coverage both to vulnerable nationals who are
not covered, as well as to refugees and migrants. It
is important to complement them with productive
inclusion plans that imply, in the case of rural areas

50
Migration from Venezuela: opportunities for Latin America and the Caribbean
still highly dependent on agriculture, coordination
with other programs aimed at strengthening
access to natural and nancial resources, technical
assistance, and marketing routes.
To advance in the consolidation of a comprehensive
social protection system that includes a social
protection floor, the following roadmap is proposed,
which is more necessary than ever in this context of
a pandemic that has highlighted the importance of
universal social protection.
u Strategic lines
1. Roadmap to guarantee access to social
protection for refugee and migrant workers and
their families, promoting a social protection
floor:
Preparation of reports with policy
recommendations, which include an analysis
of international regulations and national
legislation, barriers to access, coverage gaps
and challenges for connecting refugees and
migrants with the national social protection
system, whether contributory or non-
contributory.
Preparation of a proposal to implement a
social protection floor which guarantees
effective access to minimum income security
and essential health care throughout the
life cycle. This should review requirements,
access barriers and measures that can be
implemented in order to realise the right to
social security.
Preparation of a flexible afliation proposal for
national and foreign self-employed workers,
as well as for domestic workers.
Design of a micro insurance scheme for
handling family contingencies both in the
country of origin and destination.
Inclusion of migrant children in existing
care systems, which must be expanded and
strengthened in order to address their specic
needs.
Preparation and integration into the
comprehensive national social protection
system, progressively, of a proposal for daily
care and attention for children of migrant
parents.
Consideration of the particular situation of
migrant women and provision of solutions
to their particular needs, including access
to maternity and medical services for their
children, as well as conditional transfers for
each minor.
Safeguarding the nancial and actuarial
sustainability of the different proposals.
Promotion of effective coordination of
government institutions in general and social
security in particular to guarantee good
governance of labour migration in the area of
social security.
Promotion of the application or negotiation
and signing of social security agreements
between two or more countries, which allow
the accrual of years of services and payment
of the corresponding benets. The creation
of a single regional register of social security
contributions may be envisaged.
Review of current agreements to improve
the following principles: equal treatment,
access, conservation or transferability of
social security benets, wait times and pre-
existence.
Regional socio-economic integration strategy
51
Strengthening the capacity of trade union
organizations to offer information and
assistance services to these workers.
Promotion of minimum wage policies that
include migrant workers.
Inclusion of refugees and migrants from
Venezuela in the programs and measures
adopted by governments to meet their most
pressing needs while mobility restrictions are
in effect.
2. Roadmap to disseminate information on
accessing social security and create a culture
of social security:
Design of an action plan to strengthen the
social security culture among nationals and
refugee and migrant communities, to promote
their incorporation into a social protection
floor.
Creation of a national tripartite body to monitor
the performance of the system and propose
alternatives that ensure effective and timely
access to social security for migrants.
Implementation of community workshops
with union and community organizations to
socialise their rights and obligations under
labour legislation, health and safety at work,
as well as health and social welfare among
the communities that are the object of the
Regional Strategy.
Promotion of the ratication and application
of ILO conventions and recommendations
on social protection for refugee and migrant
workers.
Design and dissemination of informational
material on rights and obligations in matters
of social protection, and the mechanisms for
making them effective.
Design of a communication plan on the
benets of being protected against different
social contingencies.
4.7 Social cohesion
The success of the Regional strategy for socio-
economic integration will be based not only on
concrete actions aimed at the refugee and migrant
population, but also on social cohesion programs
that allow better coexistence with citizens of host
communities. In different areas of Latin America
and the Caribbean, the rapid increase in both the
Venezuelan and returned population creates a
series of risks that could constitute a threat to social
cohesion, even more so in the current context of the
COVID-19 crisis.
The increasingly visible presence of refugees and
migrants in the streets, job competition in some
sectors of the economy and, especially, in the informal
sector, as well as the increase - real or perceived -
in insecurity represent some of the factors that can
contribute to the increase in xenophobia in host
countries, especially in municipalities where there
is a strong concentration of people from Venezuela.
As a result, Venezuelan refugees and migrants face
discrimination problems in the labour markets that
prevent their process of inclusion in decent work
conditions and force them to disproportionately
enter into precarious conditions and the informal
sector (see Figure 1), where they are more at risk of
being victims of labour exploitation.
For these reasons, it is important that the countries
of the region address social cohesion as an integral
part of their responses to socioeconomic integration.

52
Migration from Venezuela: opportunities for Latin America and the Caribbean
u Current situation / obstacles
Xenophobia has increased in almost all the
countries of the region as the number of refugees
and migrants from Venezuela has grown.
Returnees, despite having the nationality of the
countries to which they return, also suffer from
issues of rejection and stigmatization.
The high rates of unemployment,
underemployment and informality in the region
have contributed to reinforcing xenophobic
sentiments, particularly among the most
vulnerable population.
The population from Venezuela faces growing
problems of discrimination, particularly in terms
of access to services and formal jobs.
Women from Venezuela suffer from dual
discrimination, rst as refugees or migrants and
second as women.
The COVID-19 epidemic has contributed to the
increase in xenophobic sentiments, as some
communities see refugees and migrants as
responsible for the spread of the virus.
u Proposal
To promote social cohesion, it is important to
implement comprehensive programs that benet both
the refugee and migrant population from Venezuela,
including returnees, and host communities. Thus,
the different programs for vocational training, job
promotion or nancial support for entrepreneurship
aimed at Venezuelans should also include a local
component for the host population, especially the
most vulnerable.
Reciprocally, given the conditions of vulnerability of a
growing part of the refugee and migrant population,
the differentiated programs to combat poverty
aimed at vulnerable populations (disabled people,
Afro-descendants, indigenous people, women
heads of households, victims of armed conflicts,
among others) should have a specic component
for refugees and migrants. In São Paolo, Brazil, the
Trabalho Novo (New Work) program, which supports
newcomers and offers them housing in municipal
shelters, Portuguese and computer classes, as well
as access to job offers, was initially designed for
residents from the streets before being extended to
the refugee and migrant population. This program
allowed hundreds of Venezuelans to gain nancial
autonomy thanks to better integration in the labour
market and the host society.
u Strategic lines
1. Design of institutional strengthening programs
at the national and local level
Work to raise awareness among public
authorities so that they better understand
the multiple reasons why Venezuelans and
returnees leave their country, as well as the
challenges and vulnerabilities they face,
depending on their personal conditions and the
environments in which they nd themselves.
Programs designed with the participation
of governments, employers’ and workers’
organizations, to promote social dialogue.
Investment in training so that the different
State services can provide better services
and more accurate information to refugees
and migrants, taking into account issues
of discrimination, xenophobia, citizen
coexistence, socio-economic and cultural
integration, among others.
Strengthening institutional capacities to
improve migration governance with a view
towards reducing irregular migration, which
tends to exacerbate xenophobic attitudes.
Regional socio-economic integration strategy
53
Design of gender-sensitive policies that
consider the different impacts of migration on
host communities.
Dissemination of information on the rights of
refugees and migrants and the mechanisms
for their enforcement, as well as on the
channels for reporting situations of gender-
based violence and workplace and sexual
harassment.
2. Carrying out awareness campaigns with host
communities to ght discrimination and
xenophobia:
Campaigns in the national and local media to
better explain the issue of forced displacement
and promote citizen coexistence, with an
emphasis on the contribution migrants make
to the development of the countries.
Need to reduce xenophobic attitudes due to
erroneous beliefs that associate the spread of
the virus to people in a situation of mobility.
Promotion of integration activities at the local
and national level, such as intercultural and
food fairs, among others.
Organization of participatory meetings and
workshops at the local level, to sensitise host
communities and jointly develop solutions
that facilitate the local integration of refugees
and migrants.
Training programs for teaching staff, to help
them sensitise students on the migration issue
and ght more effectively against xenophobia
in schools.
Sensitisation of employers’ and workers’
organizations, as well as the business
community, to prevent abuse and
discrimination problems in the workplace, and
facilitate the labour insertion of refugees and
migrants from Venezuela into local markets.

54
Migration from Venezuela: opportunities for Latin America and the Caribbean
5
Strengthen regional
cooperation mechanisms
for socio-economic
integration
Until now, the response of Latin American and Caribbean governments to the
Venezuelan migration crisis has been directed more towards national action
than regional action, although the Quito Process pursues the latter. For this
reason, it is essential that the countries of the region succeed in strengthening
cooperation mechanisms and adopting and implementing truly regional
policies, particularly in matters of socio-economic integration for the refugee
and migrant population from Venezuela, as well as for host communities. In
this sense, the outbreak of COVID-19 in the region and the negative impact
that quarantines and other social distancing measures have had on economic
activity and employment make regional cooperation even more necessary.
Regional socio-economic integration strategy
55
Regional cooperation on socio-economic integration
should, rst of all, share the best practices implemented
by the different host countries in Latin America and
the Caribbean. Through a peer review process, it is
possible to identify which of these practices should
be replicated - with needed adaptations - in other
countries. The regional cooperation framework could
also aim for Latin American and Caribbean countries
to implement regional initiatives for socioeconomic
integration, in particular in the areas of (i) human
mobility and regularization, (ii) mutual recognition of
degrees and skills, (iii) labour intermediation and (iv)
social protection.
This type of initiative would allow for better
management of the response to refugees and
migrants from Venezuela at the regional level within
a context aggravated by the COVID-19 crisis. It would
also contribute to the achievement of the objectives
of the Quito Process.
Graphic 2. Main areas of regional cooperation in socio-economic integration
Human
mobility and
regularization
Job
intermediation
Mutual
recognition of
degrees and
compentencies
Protection
social
5.1 Expand spaces for
collaboration in the areas
of human mobility and
regularization
Although the Venezuelan migratory crisis constitutes
a phenomenon of a regional dimension with
repercussions in most of the LAC countries, the
cooperation mechanisms in the area of human
mobility and the regularization of people in an
20 https://www.cancilleria.gob.ec/declaracion-de-quito-sobre-movilidad-humana-de-ciudadanos-venezolanos-en-la-region/
irregular situation have been relatively limited. In the
early years of the crisis, the countries of the region
facilitated the mobility of people from Venezuela,
particularly through a broad interpretation of
regional integration agreements, especially within
the framework of ACN, Mercosur, and CARICOM.
Thus, in the Quito Declaration on Human Mobility of
Venezuelan citizens in the Region
20
, dated September
4, 2018, the representatives of the governments
of Argentina, Brazil, Chile, Colombia, Costa Rica,
Ecuador, Mexico, Panama, Paraguay, Peru and
56
Migration from Venezuela: opportunities for Latin America and the Caribbean
Uruguay agreed, “in accordance with the national
legislation of each country, to accept expired travel
documents as identity documents of Venezuelan
citizens for immigration purposes.” In this way,
Venezuelan people were authorized to enter most
of the countries in the region without a visa, and in
some cases, without a passport.
However, with the rapid and massive increase in the
number of refugees and migrants, restrictions on
mobility have multiplied (Selee and Bolter, 2020). A
growing number of countries began to require new
entry requirements, such as: a valid passport, despite
the difculties and high cost that this represents for
the vast majority of the Venezuelan population; a visa,
which many Venezuelan people cannot afford, and
an apostilled criminal record certicate in Venezuela,
which implies additional costs and terms.
The result of these increasingly restrictive measures
is that mobility at the regional level was limited,
complicating the living conditions of the population
from Venezuela. This trend translated into a high
number of Venezuelans in an irregular situation.
According to data from the R4V Platform (2020),
around half of Venezuelan refugees and migrants
are in an irregular migratory situation. These
restrictions also contributed to creating bottlenecks
in some transit countries, particularly in Colombia,
the country with the longest land border with
Venezuela and at the same time, the most open to
entry for the Venezuelan population. Many people in
transit were stuck in the border areas when some of
the countries in the region decided to change their
entry rules. Municipalities located on the borders
between Colombia and Ecuador, Ecuador and Peru,
and Peru and Chile were particularly affected by
these bottlenecks. In this sense, the policies adopted
unilaterally by the different countries of the region,
which were reinforced by the almost generalized
closure of the borders during the COVID-19 crisis,
had negative repercussions for both the refugee
and migrant population, as well as for neighbouring
countries.
For this reason, better cooperation in the management
of migratory flows at the regional level and the
adoption of concerted regularization mechanisms
would make it possible to avoid these types of
negative effects and facilitate the socio-economic
integration of the population from Venezuela. This
implies, for example, that the main host countries
in the region adopt joint regularization programs to
avoid massive movements to countries that decide to
unilaterally make the options for regularization of the
migrant population more flexible. In this sense, the
biannual meetings of the Quito Process could be used
for the Ministries of Foreign Affairs of each member
country to assess the conditions of the population in
an irregular migratory situation and adopt concerted
regularization measures. An alternative could be
the implementation of a regional regularization
commission to examine the current situation in
detail and propose specic recommendations that
facilitate human mobility processes at the regional
level, as well as regularization mechanisms.
On the other hand, the countries of the region could
better harmonize, especially within the framework
of the Quito Process, the procedures for asylum
applications by dening common principles for the
recognition of refugee status for Venezuelans. These
could be based on the 1984 Cartagena Declaration
on Refugees, which proposes a broader denition of
refugees than the Convention Relating to the Status
of Refugees (1951) and the Protocol on the Status of
Refugees (1967). In this way, the processes of access
to refugee status would be streamlined, taking into
account the specicities of the current situation in
Venezuela.

Regional socio-economic integration strategy
57
5.2 Build a regional framework
for the mutual recognition
of degrees and skills
An essential stage in the process of socio-economic
integration of refugees and migrants is the possibility
of obtaining recognition, on the one hand, of technical
and academic qualications, and on the other, of the
job skills that they were able to acquire throughout
their schooling and professional life. In this sense,
as noted above, it is essential that the countries of
Latin America and the Caribbean relax both their
mechanisms for the recognition of degrees awarded
abroad and for the certication of skills (see Section
4.2). But this dual process could be reinforced if
the countries of the region adopted a framework of
mutual recognition of degrees and competencies.
Regarding the recognition of competencies, the
representatives of the Ministries of Labour and
international cooperation organizations, as well as
employers’ and workers’ organizations - meeting on
November 13, 2019 in Bogotá, Colombia, in support
of the Quito Process - recommended support for
“regional homologation initiatives for the certication
of labour competencies,” in collaboration with the
“Inter-American Centre for the Development of
Knowledge in Vocational Training (CINTERFOR) of
the ILO and other entities involved in this area.” In fact,
since 2015 there has been a competency certication
network that includes the entities responsible for this
process in Argentina, Brazil, Chile, Colombia, Costa
Rica, El Salvador, Ecuador, Guatemala, Honduras,
Mexico, the Dominican Republic and Uruguay
21
.
Regarding the mutual recognition of technical and /
or academic degrees, the main regional coordination
initiative is the Organization of the Andrés Bello
Agreement for Educational, Scientic, Technological
and Cultural Integration
22
, which brings together
21 https://www.oitcinterfor.org/red_certicacion
22 http://convenioandresbello.org/cab/
Bolivia, Chile, Colombia, Cuba, Ecuador , Spain,
Mexico, Panama, Paraguay, Peru, the Dominican
Republic and Venezuela. Despite the efforts towards
educational integration among these countries, there
are still no regional mechanisms for the recognition of
degrees, which explains a large part of the difculties
faced by people with technical and / or academic
degrees awarded in Venezuela.
In this context, a regional framework for the mutual
recognition of qualications and competencies
would imply that, every time a person, whatever
their nationality or immigration status, validates a
technical or academic degree in one of the countries
of the region or certies their labour competencies,
this recognition is valid in the other countries of the
region. In this way, people who decide to migrate to
another country do not have to go through all the
procedures again and can contribute more effectively
to the economies of the recipient countries. This
regional framework of mutual recognition would
benet not only the population from Venezuela, but
also any citizen of one of the member countries with
the intention of migrating within the region. It is a
mechanism that facilitates, at the same time, intra-
regional mobility and socioeconomic integration.
This dual process of mutual recognition, which
involves both the Ministries of Education (in
particular in matters of recognition of qualications)
and of Labour (together with the national institutes
of vocational training, especially for the certication
of competencies), could be implemented within
the framework of existing multilateral mechanisms
in the region (see Table 1) and on the basis of the
agreements that apply to this matter. In addition, it
is possible to provide technical assistance for the
development of a regional qualications framework,
which can be submitted to the consideration and
validation of the member countries of the Quito
58
Migration from Venezuela: opportunities for Latin America and the Caribbean
Process. This framework would constitute a common
understanding among the countries of the region of
what is expected at each level of vocational training
and, once it is validated by the participating States, it
would facilitate the labour mobility of those who have
been certied. This framework should cover, at least,
levels 1 to 5 out of 8, with level 1 being the one with
the lowest qualications; levels 2 to 4: the different
degrees of technical-professional training and levels
5 to 8: those of higher education. Level 8 corresponds
to the doctorate.
5.3 Promote labour
intermediation at the
regional level
People from Venezuela tend to be concentrated in
border areas, particularly in the case of Colombia,
and in large cities, where there are more options
for accommodation and work, although many
times they are in the informal economy and thus
are synonymous with labour exploitation and
socioeconomic vulnerability. They also choose
destinations where they already have family or
community networks that can provide support. But,
in most cases, refugees and migrants do not have
enough information about the job opportunities
that exist in the host countries and, even if they do,
they cannot always access the public employment
services programs due to their immigration status or
lack of information on these services. For this reason,
it is important that employment services can identify
the specic barriers faced by Venezuelans and
returnees in order to improve their integration into
employability routes and help them access decent
jobs, taking into account the needs of the different
countries.
It is possible that the skills that Venezuelans and
returnees bring with them are not required in the
host country or that the absorption capacity of
the labour market is insufcient, but that they can
be used in other countries of the region. For this
reason, a reinforcement of cooperation between the
different public employment services in LAC can
contribute signicantly to a better labour inclusion of
the population from Venezuela. In addition, it would
allow better integration into the labour markets of the
region and favour intra-regional labour mobility.
Among the recommendations to the representatives
of the Ministries of Labour and international
cooperation organizations, as well as to the
employers and workers mentioned previously, is
the promotion of “the initiative for the Integration
of Public Employment Services of the Latin
American Region and the Caribbean among the
interested countries.” This initiative aims precisely at
exchanging job vacancies, having more information
on job opportunities, facilitating labour relations by
taking advantage of the skills of workers, and creating
an international mobility route in the region.” It also
highlights the need to strengthen the operation and
response of these services.
Regional cooperation on job placement implies
that databases are shared on job vacancies in
each country, as well as on the population seeking
employment, including refugees and migrants. To
better understand where job opportunities are, a
common system for monitoring the situation of labour
markets at the local level can be adopted in each
country, based on indicators such as unemployment
rates, the size of the informal economy and the
business climate (Bahar, Dooley and Huang, 2018).
In the same perspective, it is important that the
providers of the different employment agencies, both
public and private, work with business associations
to identify the skills needed in each country and share
them with other countries in the region. An initiative
of this nature demands a certain homogeneity
between the different computer platforms of the
public employment services of the countries, at the
same time that it requires regulations that allow
them this socialization.
Regional socio-economic integration strategy
59
5.4 Adopt regional social
protection mechanisms
Access to social protection is a key component of
the process of socioeconomic integration of the
refugee and migrant population (see Section 4.6).
For this reason, regional cooperation should aim to
strengthen regional social protection mechanisms.
This implies that, through better coordination of
national legislation, refugees and migrants benet
from a social protection floor that guarantees them,
throughout their life cycle and whatever their level of
qualication, effective access to minimum income
security and health care, in accordance with the
Social Protection Floors Recommendation of 2012
(No. 202) and the ILO Social Security (Minimum
Standards) Convention of 1952 (No. 102). On the
other hand, the Venezuelan migratory crisis shows
the importance not only of integrating this population
into national social protection systems, but also of
consolidating the portability of rights at the regional
level.
In fact, the lack of an instrument for the coordination
of social security legislation (bilateral, multilateral or
Ibero-American agreement) that allows the accrual
of services and payment of social security benets
translates into difculties in preserving the rights in
progress acquisition or allowing the portability of
acquired rights. Even in the presence of agreements
that coordinate social security legislation or allow
portability, certain categories of workers do not have
access to the different benets, despite having a
formal employment relationship (e.g., temporary
migrant workers).
In this sense, one of the 23 objectives agreed to
within the framework of the Global Compact for
Safe, Orderly and Regular Migration (UN, 2018a) is:
“Establish mechanisms for the portability of social
security and the benets acquired”. The objective is
for people who work in the formal sector to be able
to add the contribution periods in the different social
security systems of all the countries where they
have contributed and to access the corresponding
benets in the country where they are (ILO, 2018).
When the beneciaries complete the age and years
of contribution requirements, each social security
management entity will assume the contribution
periods in each country and will pay a full benet or
pro rata for the years of contributions to its system,
depending on whether it is a pension or other social
benets.
In Latin America and the Caribbean, most of the bilateral
and multilateral coordination agreements for social
security systems contemplate the transferability of
the rights and benets of the migrant population.
Such is the case of the Multilateral Agreement on
Social Security of Mercosur, the Andean Instrument
for Social Security of the ACN, the Multilateral Ibero-
American Agreement on Social Security of the OISS,
the Agreement on Social Security of CARICOM and
the Agreement on Social Security of the OECS (ILO,
2018).
However, these types of agreements only cover
nationals of the countries that have signed the
agreements and do not extend to migrants from
other countries. Hence the need to promote the
ratication of the Ibero-American Social Security
Agreement so that more countries are included in
this mechanism for portability of social security
rights. Until now, Argentina, Bolivia, Brazil, Chile,
Ecuador, Paraguay, Peru and Uruguay have ratied
this agreement, which is in force in all of them.
Although Venezuela also ratied it, it has not yet
deposited the instrument’s ratication or developed
the application protocols. This implies that, in the
case of Venezuelans, there are no mechanisms for
the portability of rights and benets when they move
from one country to another. Furthermore, portability
is limited when people migrate from one sub-region
to another (for example, from an ACN country to a
Mercosur country).
60
Migration from Venezuela: opportunities for Latin America and the Caribbean
For this reason, it is important to extend subregional
agreements and promote coordination between
national social security legislation, to guarantee
access of migrant workers and their families to
national social protection systems. It is essential
that they be included in the strategies designed
by the States to build social protection floors and
ensure, among other things, access to health care
and coverage against contingencies such as the one
currently experienced with the COVID-19 pandemic.
Likewise, it is necessary to review or sign agreements
between the countries to strengthen the portability
system, where the rights acquired in one of the
countries of the region remain in force when people
migrate to another country in the region.
The ratication and universal application of the
Ibero-American Social Security Agreement can be a
strategy for achieving this goal. This would facilitate
intra-regional mobility without being detrimental
to the social rights of the refugee and migrant
population, even when these people are not citizens
of one of the countries that are signatories of these
agreements, as is the case today with the Venezuelan
population. This implies harmonization work between
the different social protection providers, including
individually funded systems.
Regional socio-economic integration strategy
61
References
Acosta, Diego; Blouin, Cécile; Feline Freier,
Luisa (2019). La emigración venezolana:
respuestas latinoamericanas. (Venezuelan
emigration: Latin American responses) Work
papers. Fundación Carolina. At: https://
www.fundacioncarolina.es/wp-content/
uploads/2019/04/DT_FC_03.pdf
Bahar, Dany; Meagan Dooley y Cindy Huang (2018).
Integrating Venezuelans into the Colombian
labor market: Mitigating costs and maximizing
benets. A research document, Washington,
Brookings Institution. At: https://www.
brookings.edu/wp-content/uploads/2018/12/
Venezuelan-Migrants_english.pdf
Banco Interamericano de Desarrollo (2020). Factor
Trabajo. Trabajo y pensiones (Work Factor.
Work and pensions.) At: https://blogs.iadb.
org/trabajo/es/que-efectos-tendra-la-covid-
19-sobre-el-empleo-de-america-latina-y-el-
caribe/
Inter-American Development Bank (2018). Creciendo
con Productividad: Una agenda para la Región
Andina (Growing with productivity: An agenda
for the Andean Region). At: http://dx.doi.
org/10.18235/0001178
World Bank (April 22, 2020). World Bank Predicts
Sharpest Decline of Remittances in Recent
History. At: https://www.worldbank.org/
en/news/press-release/2020/04/22/
world-bank-predicts-sharpest-decline-of-
remittances-in-recent-history
Blouin, Cécile (Coordinator) (2019). Estudio sobre
el perl socio económico de la población
venezolana y sus comunidades de acogida:
una mirada hacia la inclusion (Study on the
socio-economic prole of the Venezuelan
population and its host communities: a
look towards inclusion). Lima: Instituto de
Democracia y Derechos Humanos de la
Ponticia Universidad Católica del Perú y
PADF. At: https://r4v.info/es/documents/
download/70863
Bravo M., Juan and Úzua, Sergio (2018). Working Paper
N° 48. Inmigrantes: Empleo, capital humano
y Crecimiento (Immigrants: Employment,
Human Capital and Growth). Chile: Centro
Latinoamericano de Políticas Económicas y
Sociales (CLAPES-UC). At: https://clapesuc.
cl/assets/uploads/2018/07/09-07-18-doc-
trab-48-inmigrantes-jul-2018-vf.pdf
Carcedo, Ana; María José Chaves Groh and Larraitz
Lexartza (2020), Mujeres migrantes, refugiadas
y retornadas provenientes de Venezuela:
Un estudio de sus condiciones y accesos a
medios de vida en Colombia, Ecuador y Perú
(Migrant, refugee and returnee women from
Venezuela: A study of their conditions and
access to livelihoods in Colombia, Ecuador
and Peru), UNDP.
Célleri, Daniela (2019). Situación laboral y aporte
económico de inmigrantes en el norte de
Quito-Ecuador. Una primera aproximación
cuantitativa para dialogar sobre política
pública (Labour situation and economic
contribution of immigrants in the north of
Quito-Ecuador. A rst quantitative approach to
dialogue on public policy). Ecuador: Friedrich
Ebert Stiftung. At: http://library.fes.de/pdf-
les/bueros/quito/15204.pdf
62
Migration from Venezuela: opportunities for Latin America and the Caribbean
Clemens, Michael; Cindy Huang y Jimmy Graham
(2018). The Economic and Fiscal Effects of
Granting Refugees Formal Labour Market
Access. CGD Working Paper 496. Washington,
DC: Centre for Global Development. At: https://
www.cgdev.org/publication/economic-and-
fiscal-effects-granting-refugees-formal-
labor-market-access
Economic Commission for Latin America and the
Caribbean, Spanish Agency for International
Cooperation and Ibero-American General
Secretariat (2007). Social cohesion, inclusion
and sense of belonging in Latin America and
the Caribbean. Synthesis. Santiago, Chile.
Inter-American Commission on Human Rights.
Pandemic and Human Rights in the Americas.
RESOLUTION 1/2020. At: http://www.oas.org/
en/iachr/decisions/pdf/Resolution-1-20-en.
pdf
IMF (2020), World Economic Outlook, April 2020: The
Great Lockdown, International Monetary Fund.
At: https://www.imf.org/en/Publications/
WEO/Issues/2020/04/14/weo-april-2020
Koechlin, José; Solórzano Ximena; Larco, Giovanna
y Fernández-Maldonado, Enrique (2019).
Impacto de la inmigración venezolana en
el mercado laboral de tres ciudades: Lima,
Arequipa y Piura (Impact of Venezuelan
immigration on the labour market of three
cities: Lima, Arequipa and Piura). Perú: ILO and
IOM. At: https://peru.iom.int/sites/default/
les/Documentos/IMPACTOINM2019OIM.pdf
Mercer, Hugo (2019). Integración laboral en el
sector salud de la población venezolana en
la República de Argentina (Labour integration
in the health sector of the Venezuelan
population in the Republic of Argentina).
IOM: Argentina. At: http://docs.bvsalud.org/
biblioref/2019/10/1022761/integracion_
laboral_sector_-salud_poblacion_venezolana-
republi_Aeqpy29.pdf
ILO (7 April 2020). ILO Observatory: COVID-19 and
the world of work. Second edition Updated
estimates and analysis. At: https://www.ilo.
org/wcmsp5/groups/public/---dgreports/-
--dcomm/documents/briefingnote/
wcms_740877.pdf
ILO (29 April, 2020). ILO Observatory: COVID-19
and the world of work. Third edition Updated
estimates and analysis. At: https://www.ilo.
org/wcmsp5/groups/public/---dgreports/-
--dcomm/documents/briefingnote/
wcms_743146.pdf
ILO (17-18 September 20192019). Concept Notes.
Session 2/Note 1: Employment and sustainable
enterprises. Key motors of sustained, inclusive
and sustainable economic growth, full and
productive work, and decent work for all.
ILO and UN Resident Coordinators Dialogue
on Decent Work and Economic Growth in
the context of the Future of Work in Latin
America and the Caribbean. At: https://www.
ilo.org/wcmsp5/groups/public/---americas/-
--ro-lima/documents/discussionforum/
wcms_718734.pdf
ILO (2018). Panorama Laboral Temático 4. Presente
y futuro de la protección social en América
Latina y el Caribe. Organización Internacional
del Trabajo, (Thematic Labour Overview 4.
Present and future of social protection in Latin
America and the Caribbean). International
Labour Organization, Lima, Peru. At: https://
www.ilo.org/wcmsp5/groups/public/---
americas/---ro-lima/documents/publication/
wcms_633654.pdf
ILO (2017a). World Report on Social Protection.
Universal social protection to achieve the
Sustainable Development Goals. International
Labour Organization, Geneva, Switzerland.
Regional socio-economic integration strategy
63
ILO (2017b). Global Youth Employment Trends
2017: Paths to a better working future. At:
https://www.ilo.org/wcmsp5/groups/public/-
--dgreports/---dcomm/---publ/documents/
publication/wcms_598669.pdf
ILO (2011). La inmigración laboral de sudamericanos
en Argentina (Labour immigration of South
Americans in Argentina). ILO Country Ofce for
Argentina and Ministry of Labour, Employment
and Social Security. 1st ed. Buenos Aires:
ILO. At: https://www.ilo.org/wcmsp5/groups/
public/---americas/---ro-lima/---ilo-buenos_
aires/documents/publication/wcms_bai_
pub_107.pdf
OECD/ILO (2018). How Immigrants Contribute
to Developing Countries’ Economies?
Paris, OECD Publishing. At: http://dx.doi.
org/10.1787/9789264288737-en
OECD/UNHCR (2018). Engaging with Employers
in the Hiring of Refugees: A 10-point multi-
stakeholder action plan for employers,
refugees, governments and civil society,
Paris, OECD Publishing. At: https://www.oecd.
org/els/mig/UNHCR-OECD-Engaging-with-
employers-in-the-hiring-of-refugees.pdf
World Health Organization (WHO) (2019). Preguntas
y respuestas sobre la enfermedad por
coronavirus (COVID-19) (Questions and
Answers on Coronavirus Disease (COVID-19)).
At: https://www.who.int/es/emergencies/
diseases/novel-coronavirus-2019/advice-
for-public/q-a-coronaviruses
UNDP (2020a). COVID-19 and Human Development:
Assessing the Crisis, Envisioning the Recovery,
2020 Human Development Perspectives. At:
http://hdr.undp.org/en/hdp-covid
UNDP (2020b). Early recovery responses to COVID-19
for migrants and host communities in Latin
America and the Caribbean, At: https://www.
latinamerica.undp.org/content/rblac/en/
home/library/democratic_governance/early-
recovery-responses-for-migrants-and-host-
communities-maxim.html
UNDP / Presidency of the Republic of Colombia
(2019). Estrategia de generación de ingresos
para la población migrante proveniente de
Venezuela y las comunidades de acogida
(Income generation strategy for the migrant
population from Venezuela and the host
communities). Presidency of the Republic of
Colombia, Bogotá.
Ramírez, Jacques; Linares, Yoharlis and Useche,
Emilio (2019). (Geo) Políticas migratorias,
inserción laboral y xenofobia: migrantes
venezolanos en Ecuador ((Geo) Migration
policies, labour insertion and xenophobia:
Venezuelan migrants in Ecuador). In Blouin,
Cécile. Después de la Llegada. Realidades
de la migración venezolana (After arrival.
Realities of Venezuelan migration). Lima, Perú:
Themis-PUCP. At: https://www.aacademica.
org/jacques.ramirez/22.pdf
R4V (2020). Coordination platform for refugees and
migrants from Venezuela. At: https://r4v.info/
en/situations/platform
R4V (Up to December 2019). Venezuelan Refugees
and Migrants in the Region. Latin American
and the Caribbean). At: https://r4v.info/en/
documents/download/72764
R4V (April-May 2019). Caribbean Situation Report
April-May 2019. At: https://data2.unhcr.org/
en/documents/download/70561
Salgado Bustillos, Flavio; Contreras Painemal, Carlos
y Albornoz, Lorena. (2017). La migración
venezolana en Santiago de Chile: entre la
inseguridad laboral y la discriminación. Revista
Internacional de Estudios Migratorios (RIEM).
64
Migration from Venezuela: opportunities for Latin America and the Caribbean
At: le:///C:/Users/mlxir/Downloads/2164-
6290-1-PB%20(1).pdf
Selee A. y Bolter J (2020). An Uneven Welcome:
Latin American and Caribbean Responses
to Venezuelan and Nicaraguan Migration.
Migration Policy Institute. At: https://
www.migrationpolicy.org/research/
latam-caribbean-responses-venezuelan-
nicaraguan-migration
Simoes, G.; Cavalcanti, L.; Moreira, E.; Camargo, J.
(2017). Executive summary. Socidemographic
and labour prole of Venezuelan immigration in
Brazil. National Immigration Council. Brasìlia,
DF: CNIg. At: https://portaldeimigracao.mj.gov.
br/images/publicacoes-obmigra/Executive_
Summary_OBMigra_1.pdf
Tincopa, Gabriel (Lead researcher). (May 2019).
Capacidades y competencias de mujeres
venezolanas residentes en Perú. Evaluación
rápida de mercado (Capacities and
competencies of Venezuelan women residing
in Peru. Quick market assessment). Perú:
CARE. At: http://trabajodigno.pe/wp-content/
uploads/2019/08/Investigaci%C3%B3n-
Inmigraci%C3%B3n-Venezuela-CARE-PERU.
pdf
UN (2020). A UN framework for the immediate socio-
economic response to COVID-19, United
Nations, New York. At: https://unsdg.un.org/
resources/un-framework-immediate-socio-
economic-response-covid-19
UN (2018a). Global Compact for Safe, Orderly and
Regular Migration, United Nations, New York.
At: https://www.un.org/en/ga/search/view_
doc.asp?symbol=A/RES/73/195
UN (2018b). Global Compact on Refugees, United
Nations, New York. At: https://www.unhcr.org/
gcr/GCR_English.pdf
UN (2015). Transforming our world: the 2030 Agenda
for Sustainable Development, United Nations,
New York. https://sustainabledevelopment.
un.org/content/documents/21252030%20
Agenda%20for%20Sustainable%20
Development%20web.pdf
UNCTAD/IOM/UNHCR (2018). Policy Guide on
Entrepreneurship for Migrants and Refugees,
United Nations Conference on Trade and
Development, Geneva. At: https://unctad.org/
en/PublicationsLibrary/diae2018d2_en.pdf
UNHCR (2019). Global trends forced displacement
in 2019. At: https://www.unhcr.org/
globaltrends2019/
World Bank (2020). Migration from Venezuela to
Latin America: COVID-19 Pandemic Impacts
and Needs, Presentation 14 May, 2020.
DTM reports
IOM (September 2018). Monitoring Venezuelan
Citizen’s Presence: Trinidad and Tobago.
Round 1: :https://reliefweb.int/sites/reliefweb.
int/files/resources/DRAFT_TT_REPORT_
SEP2018_201810291833.pdf
IOM (October 2018). Displacement Tracking Matrix:
Guyana. Round 2: https://reliefweb.int/sites/
reliefweb.int/les/resources/69567.pdf
IOM (May 2019). Displacement Tracking Matrix:
Guyana: https://reliefweb.int/sites/reliefweb.
int/les/resources/69616.pdf
IOM (July 2018). Displacement Tracking Matrix in
Chile. DTM. Round 1: https://r4v.info/es/
documents/download/72763/reliefweb.int/
sites/reliefweb.int/les/resources/66852.pdf
IOM (July to November 2018) Displacement Tracking
Matrix of the Venezuelan Population in Costa
Rica.
Regional socio-economic integration strategy
65
IOM (October 2018). Displacement Tracking Matrix
of the Venezuelan Population in Uruguay.
DTM. Round 1: https://migration.iom.int/
reports/uruguay-%E2%80%94-monitoreo-
de-flujo-de-poblaci%C3%B3n-venezolana-1-
octubre-2018-0
IOM (December 2018). Displacement Tracking Matrix.
Understanding the Venezuelan Population
Flow in the Dominican Republic: https://www.
refworld.org.es/pdd/5ce48bc04.pdf
IOM (December 2018). Displacement Tracking Matrix
of the Venezuelan Population in Mexico. DTM.
Round 1: https://www.mexico.iom.int/sites/
default/files/ArchivosDTM/Reporte%20OIM.
pdf
IOM (December 2018). DTM Results Phase IV in
Colombia. Implemented in border areas
with Venezuela and intermediate cities:
https://reliefweb.int/sites/reliefweb.int/les/
resources/69537_0.pdf
IOM (December 2018). Displacement Tracking Matrix
of the Venezuelan Population in Argentina.
DTM. Round 3: https://robuenosaires.iom.
int/sites/default/files/Informes/DTM/DTM_
Ronda_3.pdf
IOM (April 2019). Displacement Tracking Matrix of the
Venezuelan Population in Brazil. DTM. Round
4: https://reliefweb.int/sites/reliefweb.int/
files/resources/brazil_mfp%20venezolana_
r4.pdf
IOM (June 2019). Displacement Tracking Matrix of
the Venezuelan Population in Ecuador. DTM.
Round 5. https://migration.iom.int/system/
tdf/reports/REPORTE%20DTM%20R5%20
ECUADOR.pdf?le=1&type=node&id=6282
IOM (July 2019). Displacement Tracking Matrix
of the Venezuelan Population in Paraguay.
DTM: https://reliefweb.int/sites/reliefweb.int/
files/resources/DTM_REPORT_PARAGUAY_
Rev_02setIB-2.pdf
IOM (September 2019). Displacement Tracking
Matrix of the Venezuelan Population in Peru.
DTM. Report 6: https://reliefweb.int/sites/
reliefweb.int/les/resources/71522.pdf

